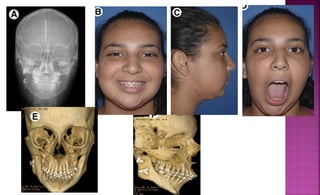
This document describes surgical techniques for treating TMJ ankylosis in children, including:
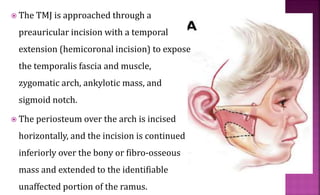
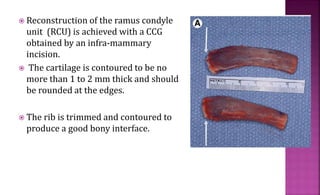
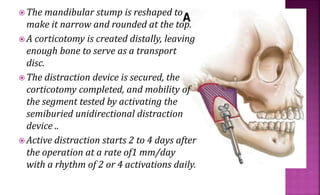
1. Excising the ankylotic mass through a preauricular incision and reconstructing the ramus condyle unit with either a costochondral graft or distraction osteogenesis.
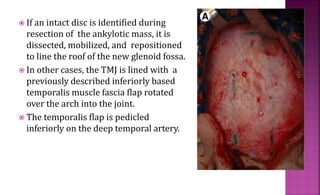
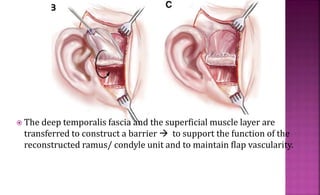
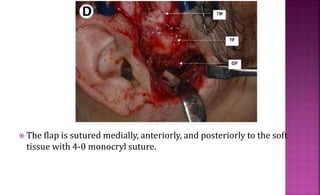
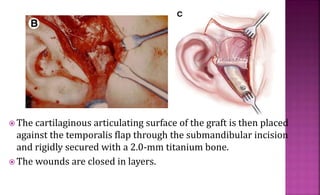
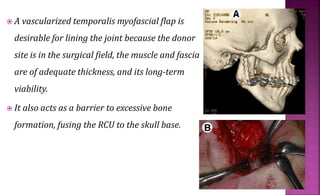
2. Lining the glenoid fossa with a vascularized temporalis fascia flap to prevent reankylosis.
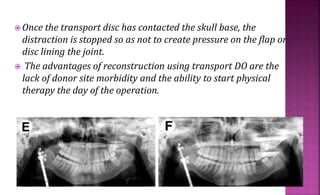
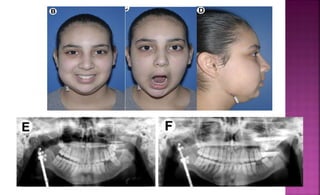
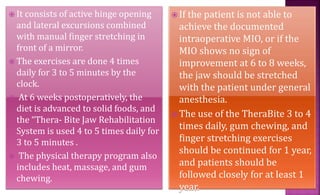
3. An intensive post-operative physical therapy regimen to regain jaw mobility.















































![TMJ ]Treatment options.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/tmjtreatmentoptions-230709162513-43034832-thumbnail.jpg?width=640&height=640&fit=bounds)
























