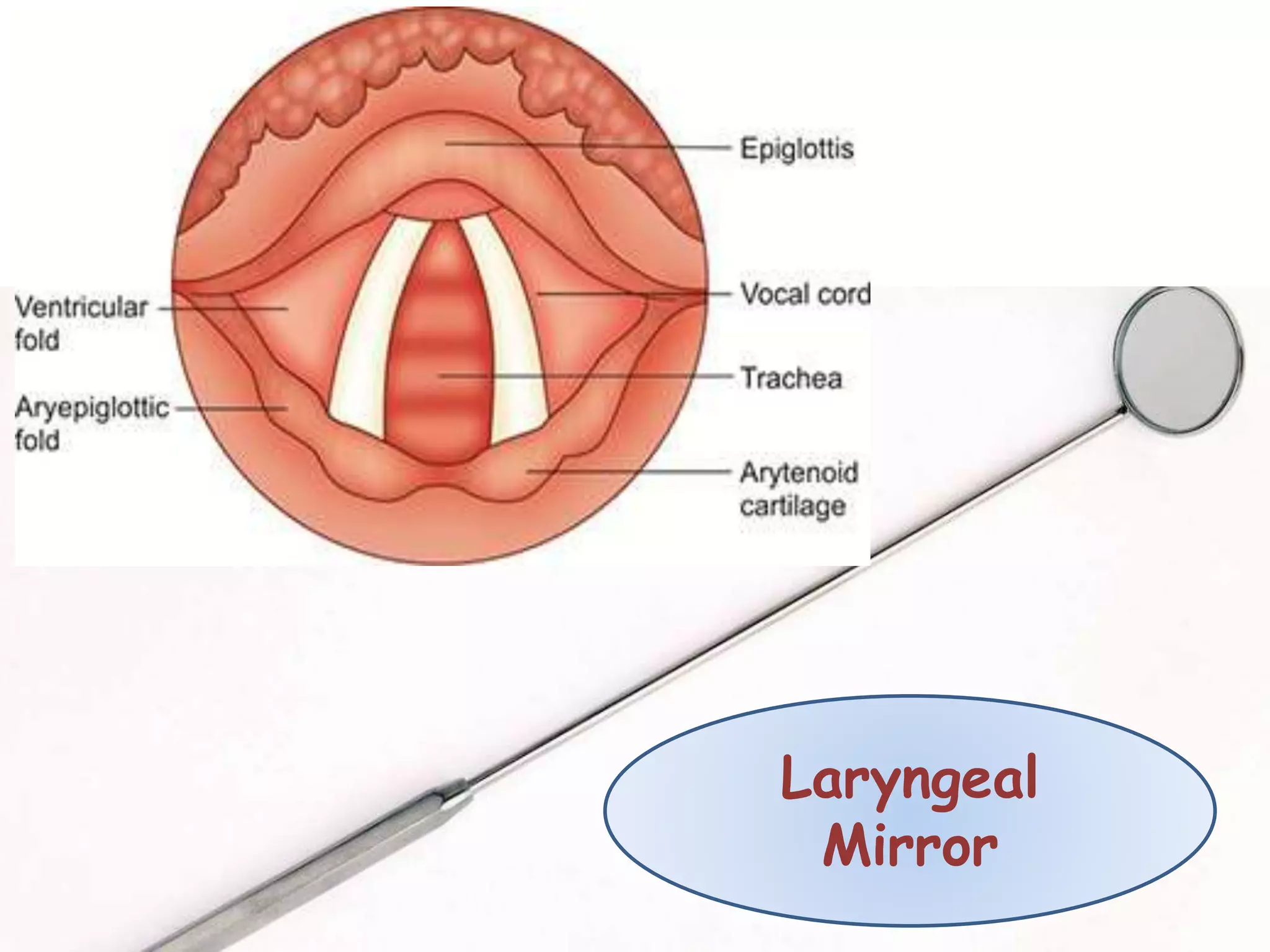
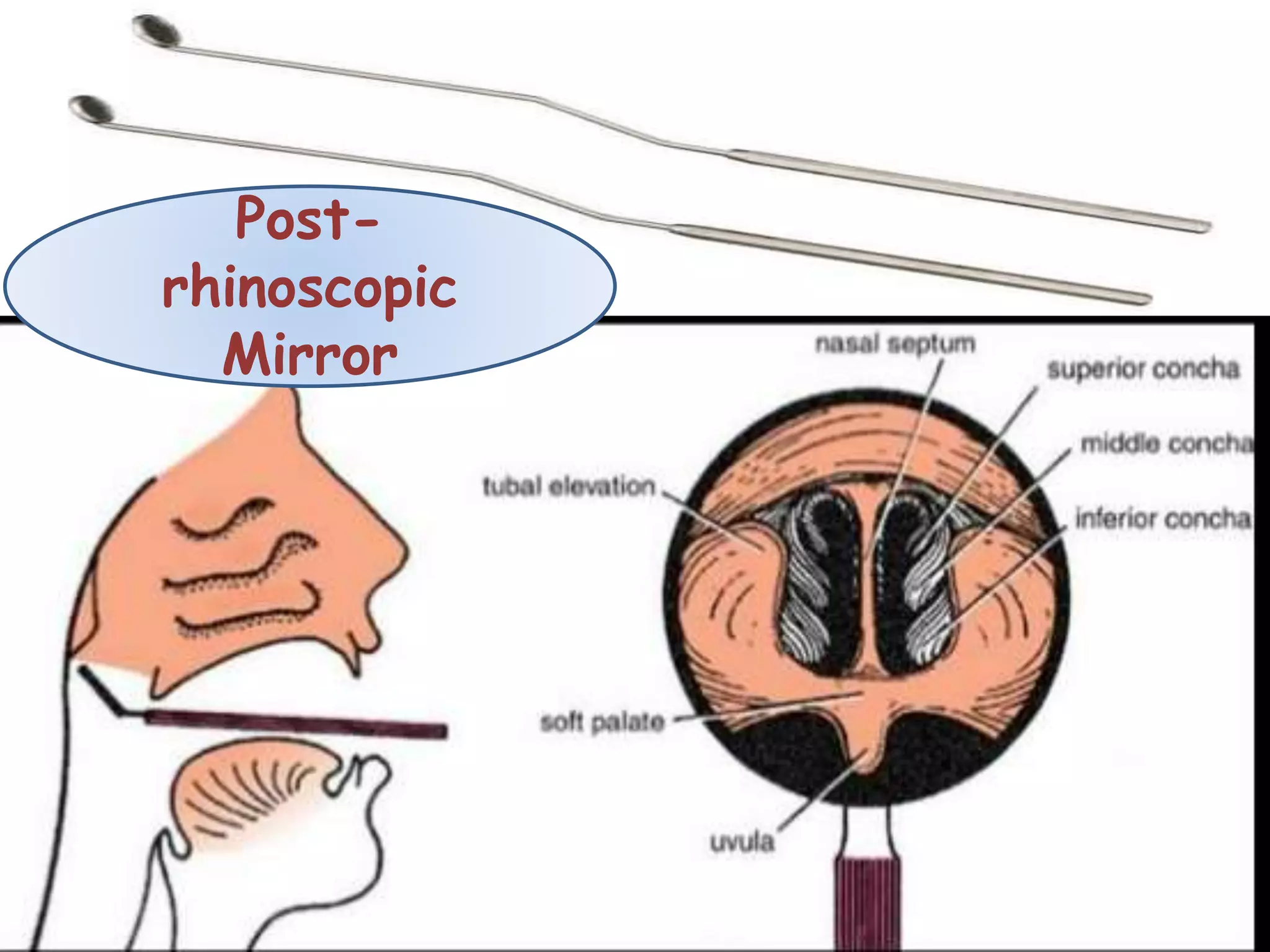
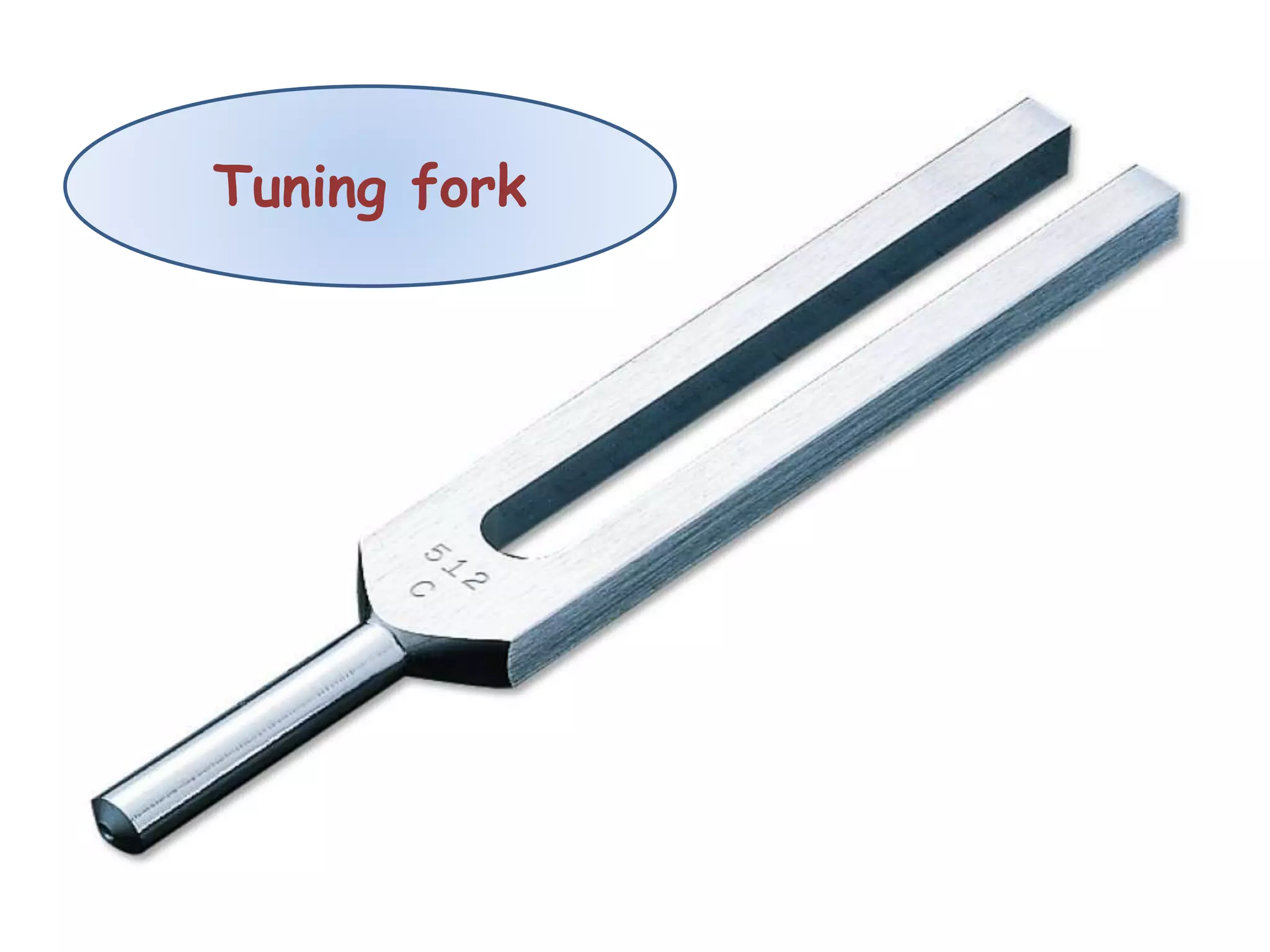
The document summarizes the examination of the nose and paranasal sinuses. It describes various instruments used in the examination like speculums, mirrors, and probes. It details the different parts of the examination including inspection of the external nose, anterior and posterior rhinoscopy, and tests to evaluate nasal patency and smell. Common complaints, nasal obstructions, and findings related to the sinuses are also outlined. The examination aims to thoroughly evaluate the nose and related structures.













































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)


















