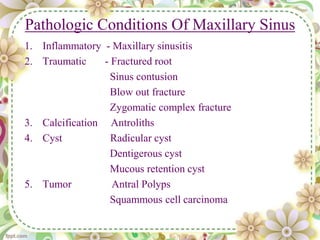
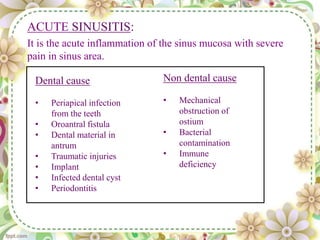
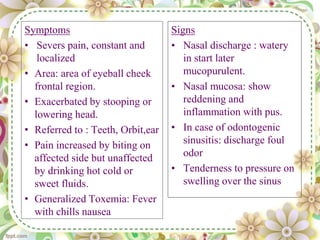
The document provides information about the maxillary sinus:
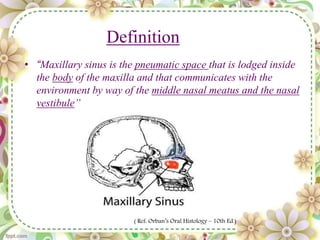
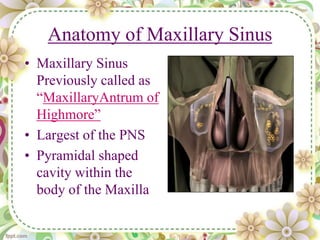
1. The maxillary sinus is an air-filled space located within the body of the maxilla bone that communicates with the nasal cavity.
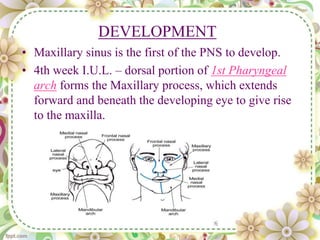
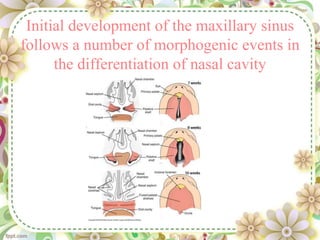
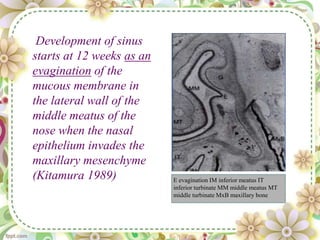
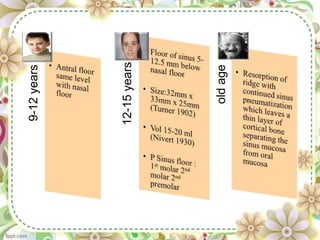
2. It develops beginning at 12 weeks of gestation as an outpocketing of the nasal epithelium. The maxillary sinus is the first paranasal sinus to develop.
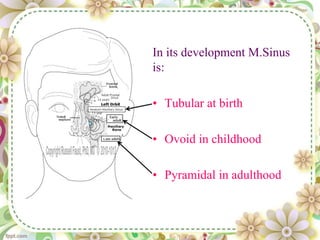
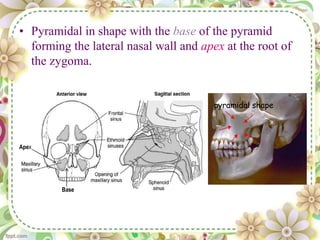
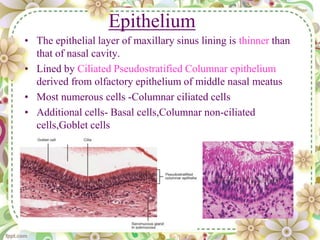
3. In adults, it has a pyramidal shape with its base forming the lateral nasal wall and its apex near the zygomatic bone. It is lined by ciliated pseudostratified columnar epithelium and contains seromucous glands.



![REFERNCES
• B D CHAURASIA’S HUMAN ANATOMY
• THE MAXILLARY SINUS AND ITS DENTAL IMPLICATION
MCGOWEN, BAXTER & JAMES;THE MAXILLARY SINUS.
• ORABANS ORAL HISTOLOGY AND EMBRYOLOGY
• DISEASES OF EAR, NOSE & THROAT ; P L DHINGRA
• JAMES K AVERY
ESSENTIALS OF ORAL HISTOLOGY,& EMBRYOLOGY
• NEELIMA MALIK; TEXTBOOK OF ORAL & MAXILLOFACIAL SURGERY.
• TEXTBOOK ORAL MEDICINE ;ANIL GHOMS
• ORAL RADIOLOGY : WHITE AND PHAROAH
• ORIGINAL ARTICLE The Location of Maxillary Sinus Ostium and Its
Clinical Application (L. C. Prasanna • H. Mamatha) [Indian J Otolaryngol
Head Neck Surg October–December 2010) 62(4):335–337]
• Endo-antral Syndrome and various endodontic complication(JOE May
1999 vol 25(5) 389-393](https://image.slidesharecdn.com/finalmaxillarysinusseminar-150419074244-conversion-gate02/85/maxillary-sinus-seminar-62-320.jpg)




































































