Downloaded 155 times
![DEVELOPMENT
It is the first paranasal sinus to develop.
Initial development of sinus follows a number of
morphogenic events in the differentiation of the
nasal cavity in early gestation(about 32 mm
crown-rump length [CRL] in an embryo.)
Horizontal shift of the Palatal Shelves &
subsequent fusion with one another](https://image.slidesharecdn.com/pragya-170511062633/85/Maxillary-sinus-13-320.jpg)


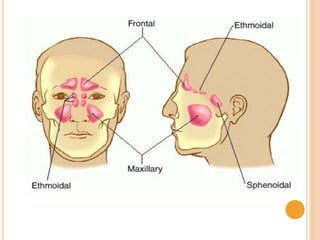
The document provides an overview of the maxillary sinus, including its anatomy, development, and clinical significance. It discusses the sinus's definition, structure, blood and nerve supply, and functions, as well as potential clinical issues such as infections and dental complications. Additionally, it covers developmental anomalies linked to various syndromes impacting the maxillary sinus.











































































![7.__Developing_a_Research_Proposal[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/7-260131073037-df92dd7d-thumbnail.jpg?width=640&height=640&fit=bounds)