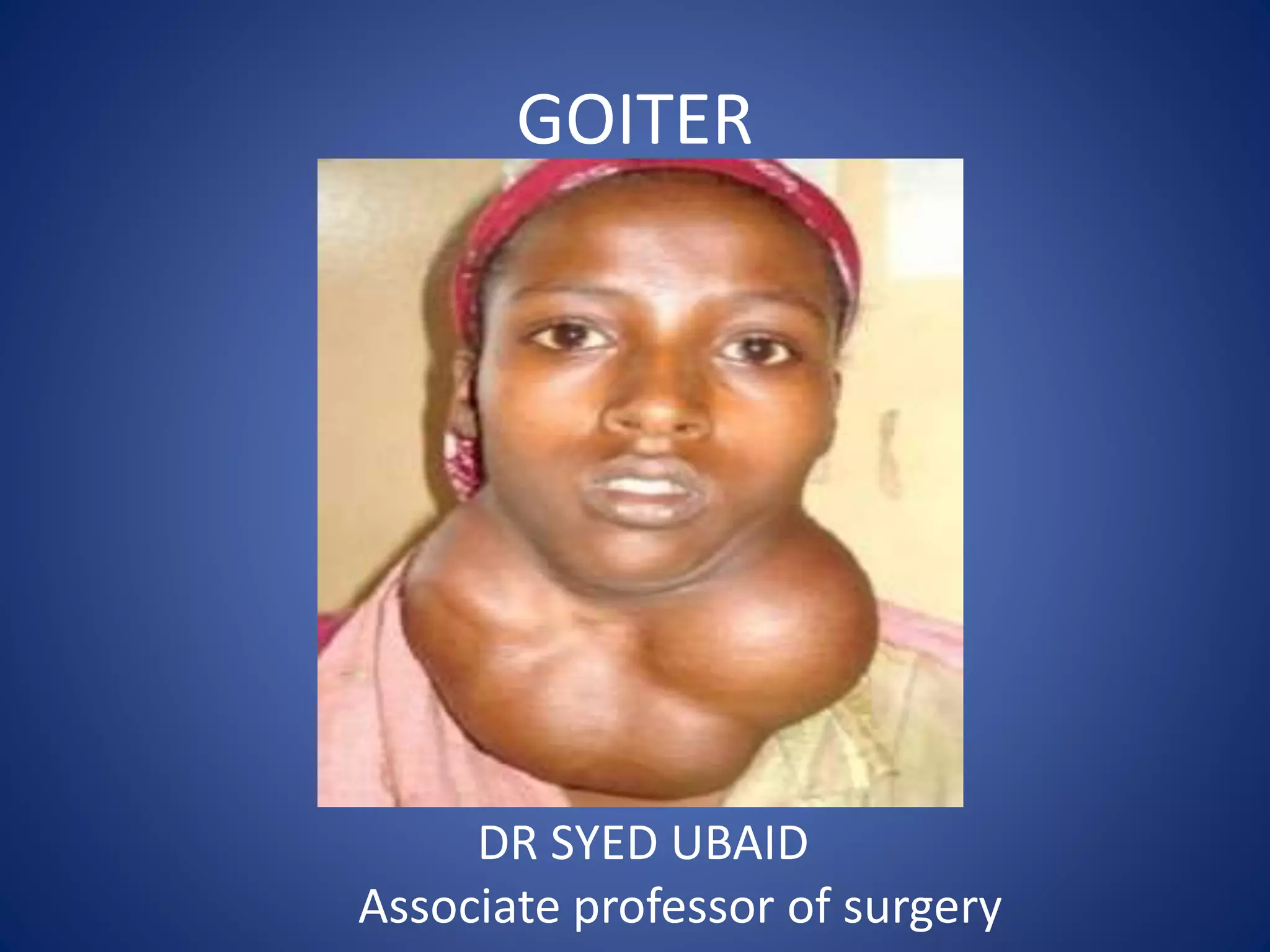
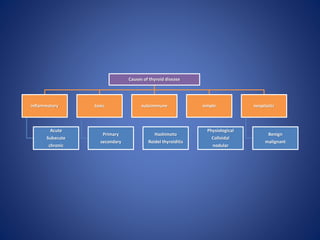
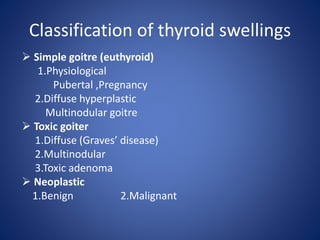
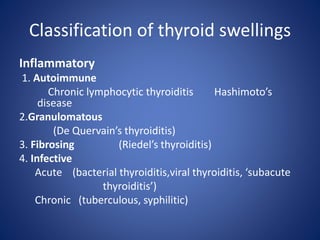
This document provides information about goiter (enlargement of the thyroid gland). It begins by defining goiter and discussing the causes, which can be inflammatory, toxic, autoimmune, or physiological. It then classifies thyroid swellings and discusses the pathophysiology, clinical presentation, investigations and treatment of simple goiter. It also discusses hypothyroidism, its causes, symptoms, diagnosis and treatment. Finally, it discusses hyperthyroidism/toxic goiter, the causes including Graves' disease, and discusses Graves' disease in more detail.




















































![THYROID_GLAND[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/thyroidgland1-231005071359-bdb08841-thumbnail.jpg?width=640&height=640&fit=bounds)













































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

