Downloaded 75 times

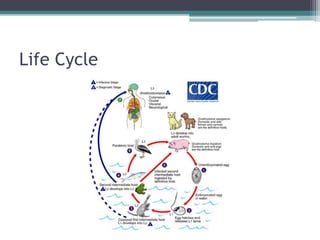

Gnathostoma spinegerum is a parasitic roundworm that can infect humans. It is commonly found infecting dogs, cats and other carnivores in parts of Asia, including Japan, China, Thailand, and the Philippines. People usually become infected by consuming raw or undercooked freshwater fish that contain the worm larvae. The adult worms live coiled in the intestinal walls of definitive hosts. The larvae can cause a migrating skin infection or visceral larva migrans if they enter the human host. Diagnosis involves identifying the worm after removal from tissues or doing intradermal tests using worm antigen to detect an immune response.














































![[Parasitologia] atlas de parasitologia color (en)](https://cdn.slidesharecdn.com/ss_thumbnails/parasitologiaatlasdeparasitologia-coloren-140923211541-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)












































