Downloaded 666 times















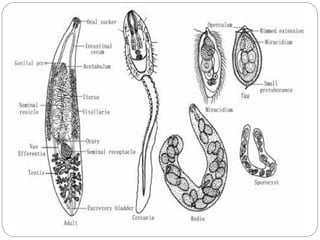























1) Clonorchis sinensis is a food-borne trematode parasite known as the oriental liver fluke. It infects over 30 million people in Asia, mainly in China and Taiwan. 2) It has a complex life cycle involving freshwater snails and fish as intermediate hosts. Humans become infected by eating raw or undercooked freshwater fish containing the infective metacercariae. 3) Most infections are asymptomatic but can cause liver inflammation and damage. Heavy infections may lead to complications like cholangitis, cholecystitis and liver cirrhosis. Diagnosis involves finding characteristic eggs in stool or bile. Praziquantel treatment is highly effective.






























































































