DEFINITION
➢Glaucoma is agroup of eye conditions that can cause
blindness by causing damage to the optic nerve by the
effect of raised intraocular pressure on the optic nerve
head
➢Most common risk factor – raised intraocular pressure (IOP)
➢The intraocular pressure depends on the balance between
production and the drainage of the aqueous humor
3.
EYE ANATOMY
Structures involved:-
1.Ciliary body(production of aq. humour)
2.Angle of anterior chamber(drainage of aqueous humour)
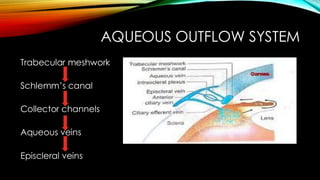
3.Aqueous outflow system
4.
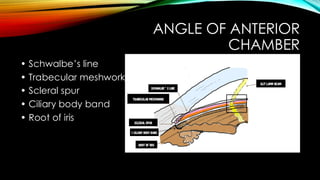
ANGLE OF ANTERIOR
CHAMBER
•Schwalbe’s line
• Trabecular meshwork
• Scleral spur
• Ciliary body band
• Root of iris
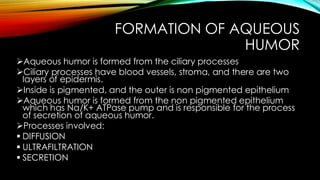
FORMATION OF AQUEOUS
HUMOR
➢Aqueoushumor is formed from the ciliary processes
➢Ciliary processes have blood vessels, stroma, and there are two
layers of epidermis.
➢Inside is pigmented, and the outer is non pigmented epithelium
➢Aqueous humor is formed from the non pigmented epithelium
which has Na/K+ ATPase pump and is responsible for the process
of secretion of aqueous humor.
➢Processes involved:
▪ DIFFUSION
▪ ULTRAFILTRATION
▪ SECRETION
7.
OUTFLOW OF AQUEOUSHUMOR
90%- CONVENTIONAL/TRABECULAR FLOW
10%- UVEO-SCLERAL FLOW
8.
CONVENTIONAL OUTFLOW
The trabecularaqueous outflow refers to the process by which aqueous humor, the fluid
inside the eye, drains from the anterior chamber to maintain intraocular pressure (IOP).
Here's a brief explanation in steps:
1.Aqueous Humor Production: The aqueous humor is produced by the ciliary body,
located behind the iris. This fluid helps nourish the eye and maintains pressure.
2.Flow into the Anterior Chamber: Once produced, the aqueous humor flows through
the pupil into the anterior chamber of the eye (the space between the cornea and
the iris).
3.Trabecular Meshwork: The aqueous humor drains through the trabecular meshwork, a
spongy tissue located at the junction of the cornea and the iris (the angle of the
anterior chamber).
4.Drainage into Schlemm's Canal: The fluid then passes through the trabecular
meshwork into the Schlemm's canal, a circular vessel that collects the aqueous
humor.
5.Return to Bloodstream: From Schlemm's canal, the aqueous humor is drained into the
bloodstream via collector channels, ultimately returning to the body's circulation.
9.
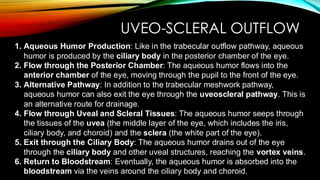
UVEO-SCLERAL OUTFLOW
1. AqueousHumor Production: Like in the trabecular outflow pathway, aqueous
humor is produced by the ciliary body in the posterior chamber of the eye.
2. Flow through the Posterior Chamber: The aqueous humor flows into the
anterior chamber of the eye, moving through the pupil to the front of the eye.
3. Alternative Pathway: In addition to the trabecular meshwork pathway,
aqueous humor can also exit the eye through the uveoscleral pathway. This is
an alternative route for drainage.
4. Flow through Uveal and Scleral Tissues: The aqueous humor seeps through
the tissues of the uvea (the middle layer of the eye, which includes the iris,
ciliary body, and choroid) and the sclera (the white part of the eye).
5. Exit through the Ciliary Body: The aqueous humor drains out of the eye
through the ciliary body and other uveal structures, reaching the vortex veins.
6. Return to Bloodstream: Eventually, the aqueous humor is absorbed into the
bloodstream via the veins around the ciliary body and choroid.
CONGENITAL/DEVELOPMENTAL
GLAUCOMA
➢ Occurs whena congenital defect in the angle of the anterior chamber obstructs the outflow of the aqueous humor.
➢ If it remains untreated causes damage to the optic nerve and blindness.
TRUE CONGENITAL GLAUCOMA
▪ Occurs when IOP increases during intrauterine period.
▪ child is born with ocular enlargement.
▪ occur in 40% of cases.
INFANTILE GLAUCOMA
▪ Occurs during third birthday
▪ occurs in about 10% of cases
▪ due to developmental trabecular dysfunction
JUVENILE GLAUCOMA
▪ hereditary autosomal dominant glaucoma
▪ Occurs during 3 to 16 years of life
▪ occurs in about 10% of cases
14.
CLINICAL FEATURES
➢Lacrimation- Excessivetearing due to irritation, infection, or obstruction of
Lacrimal gland
➢Photophobia- Abnormal sensitivity to light
➢Corneal oedema- Swelling of the cornea due to fluid accumulation
➢Raised IOP
➢Eyes become MYOPIC
➢Corneal diameter more than 13 mmhg
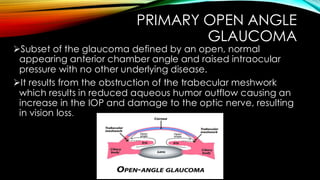
PRIMARY OPEN ANGLE
GLAUCOMA
➢Subsetof the glaucoma defined by an open, normal
appearing anterior chamber angle and raised intraocular
pressure with no other underlying disease.
➢It results from the obstruction of the trabecular meshwork
which results in reduced aqueous humor outflow causing an
increase in the IOP and damage to the optic nerve, resulting
in vision loss.
17.
RISK FACTORS
▪ IOP(High or difference of IOP between two iris is >4mmhg)
▪ Age>40 yrs
▪ Positive family history
▪ High myopia
▪ Genes responsible: myocilin-MYOC gene
Optineurin gene-OPTN gene
WTR-36
18.
PATHOGENESIS
1. Increased IntraocularPressure (IOP)
Impaired Aqueous Humor Outflow: In POAG, the primary cause of elevated IOP is the impaired drainage of
aqueous humor through the trabecular meshwork. This meshwork becomes less efficient, leading to reduced
outflow.
Trabecular Meshwork Dysfunction: Over time, the trabecular meshwork may become clogged or its cells may
become dysfunctional, further reducing the outflow of aqueous humor.
The increased resistance to aqueous humor drainage leads to a build-up of fluid inside the eye, raising IOP, which
can damage the optic nerve.
2. Optic Nerve Damage
Mechanisms of Damage: Elevated IOP can cause mechanical damage to the optic nerve head, which is where
the optic nerve fibers exit the eye. The pressure can lead to ischemia (reduced blood supply) and axonal injury
(damage to the nerve fibers), impairing the nerve’s ability to transmit visual information to the brain.
Optic Nerve Cupping: Over time, the pressure can cause optic disc cupping, where the central portion of the
optic disc (where the nerve fibers enter) becomes more hollowed out or "cupped." This is a hallmark of glaucoma.
3. Retinal Ganglion Cell Death
The increased IOP and damage to the optic nerve lead to apoptosis (programmed cell death) of the retinal
ganglion cells, which are responsible for transmitting visual information from the retina to the brain.
As the retinal ganglion cells die, there is progressive loss of the visual field, starting from the peripheral vision.
19.
CLINICAL FEATURES
➢Headache/eye ache
➢Visualacuity is normal in the initial stage
➢Colour vision is not affected
➢Visual field deficit
➢Corneal Edema
➢Loss of Peripheral vision
➢Increased IOP
20.
OCULAR HYPERTENSION
• RaisedIOP
• No fundus findings
• No visual field defects
➢It is a risk factor of glaucoma but does not always lead to it.
➢The management includes monitoring and if necessary
lowering the IOP to prevent glaucoma progression.
21.
NORMAL TENSION GALUCOMA
•IOP is normal
• Fundus changes present
• Visual field defect present
• It is associated with vascular theory of axonal loss
➢It is a subtype of POAG.
➢Treatment aims to further lower IOP using topical
hypotensive agents like prostaglandin analogs.
22.
MANAGEMENT
1. Prostaglandin analogues: Latanoprost, Travoprost
2. Topical beta blockers: Timolol maleate, Betaxolol, Levobunolol
3. Adrenergic drugs : Epinephrine hydrochloride and dipivefrin hydrochloride,
Brimonidine
4. Carbonic anhydrase inhibitors:
Topical carbonic anhydrase inhibitors like Dorzolamide or Brinzolamide and Oral
carbonic anhydrase inhibitors like acetazolamide and methazolamide.
5. Miotics : Pilocarpine
6. Hyperosmotic agents : Mannitol
23.
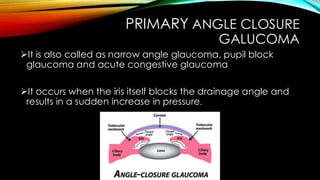
PRIMARY ANGLE CLOSURE
GALUCOMA
➢Itis also called as narrow angle glaucoma, pupil block
glaucoma and acute congestive glaucoma
➢It occurs when the iris itself blocks the drainage angle and
results in a sudden increase in pressure.
24.
PATHOGENESIS
1. Narrowing orClosure of the Anterior Chamber Angle:
The anterior chamber angle (where the cornea and iris meet) becomes narrowed or
completely closed, obstructing the drainage of aqueous humor through the trabecular
meshwork.
This can be caused by pupillary block (where the iris is pushed forward, blocking fluid
movement from the posterior to the anterior chamber).
2. Increased Intraocular Pressure (IOP):
As aqueous humor cannot drain properly, IOP rises, which can lead to optic nerve damage and
vision loss if untreated.
3. Pupillary Block Mechanism:
In pupillary block, fluid builds up behind the iris and pushes it forward, further obstructing the
drainage angle and worsening the IOP increase.
4. Acute Angle-Closure Crisis:
In some cases, the angle can suddenly close, causing an acute rise in IOP, leading to pain,
blurred vision, nausea, and potential blindness if not treated quickly.
25.
CLINICAL FEATURES
▪ Painand redness in eyes
▪ Increased IOP
▪ Blurred vision
▪ Headache and nausea
▪ Vomiting
▪ Oedematous cornea
▪ Decreased visual acuity
26.
TREATMENT
• IV Acetazolamide500mg &/or IV Mannitol
• Topical pilocarpine 2%
• Topical beta-blockers- e.g. timolol, Betaxolol
• Alpha-2 agonists- e.g. Brimonidine
• Peripheral laser iridotomy (YAG PI)
- Hole made directly in periphery of iris allowing
aqueous humor to drain directly from posterior chamber into
region of trabecular meshwork
27.
CHRONIC ANGLE CLOSURE
GALUCOMA
➢Itis a type of glaucoma where the drainage angle in the
eye becomes partially blocked over time, causing a gradual
increase in eye pressure which can lead to optic nerve
damage and vision loss, often with minimal or no noticeable
symptoms
28.
SECONDARY GLAUCOMA
Depending uponthe mechanism of rise in IOP
1. Secondary open angle glaucoma
2. Secondary angle closure glaucoma
Depending upon the causative primary disease
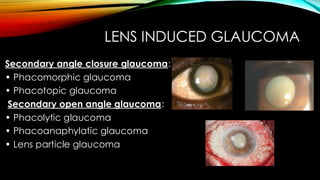
1. Lens induced (photogenic) glaucoma
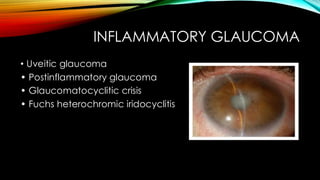
2. Inflammatory glaucoma
3. Neovascular glaucoma
4. Glaucoma associated with iridocorneal endothelial syndromes
5. Pseudo exfoliative glaucoma
6. Glaucoma in aphakia
7. Corticosteroid induced glaucoma
8. Malignant glaucoma
9. Traumatic glaucoma
10. Pigmentary glaucoma
11. Glaucoma associated with intraocular tumours
29.
DEFINITION OF SECONDARY
GLAUCOMA
➢Secondaryglaucoma occurs as a result of diseases within the eyes
such as inflammation, haemorrhage, previous surgeries, diabetes, and
steroid medication etc
➢The major types include:
▪ LENS INDUCED GLAUCOMA
▪ INFLAMMATORY GLAUCOMA
▪ GLAUCOMA IN APHAKIA/PSEUDOPHAKIA
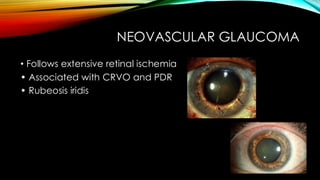
▪ NEUROVASCULAR GLAUCOMA
▪ STEROID INDUCED GLAUCOMA
▪ MALIGNANT GLAUCOMA
▪ TRAUMATIC GLAUCOMA
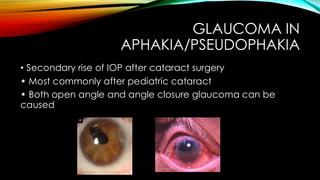
GLAUCOMA IN
APHAKIA/PSEUDOPHAKIA
• Secondaryrise of IOP after cataract surgery
• Most commonly after pediatric cataract
• Both open angle and angle closure glaucoma can be
caused
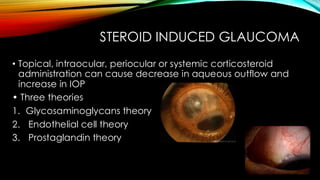
STEROID INDUCED GLAUCOMA
•Topical, intraocular, periocular or systemic corticosteroid
administration can cause decrease in aqueous outflow and
increase in IOP
• Three theories
1. Glycosaminoglycans theory
2. Endothelial cell theory
3. Prostaglandin theory
35.
MALIGNANT GLAUCOMA
• Alsocalled ciliovitreal block
• Normal flow of aqueous is blocked at the level of the ciliary
body, lens or anterior vitreous face , causing misdirection of
aqueous humor posteriorly into vitreous
36.
TRAUMATIC GLAUCOMA
• Inflammatoryglaucoma due to iridocyclitis
• Glaucoma due to intraocular haemorrhage
• Lens induced glaucoma
• Angle closure due to peripheral anterior synechiae.