This document provides an outline for a lecture on anesthesia implications for elderly patients. It discusses the normal age-related physiological changes in several body systems and how they impact anesthesia considerations. Some key points include:
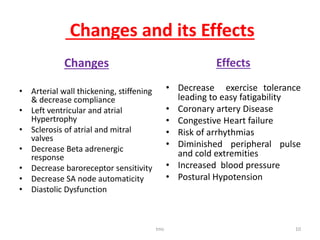
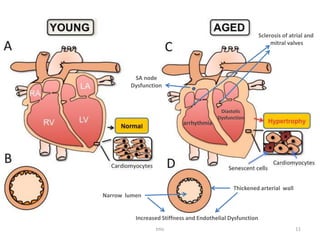
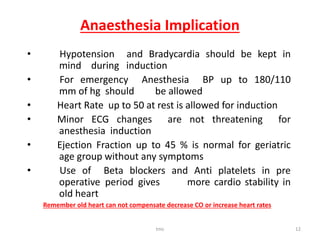
- The cardiovascular system shows decreased cardiac output, increased blood pressure, and reduced beta receptor response with age. This increases risks of hypotension, arrhythmias, and heart failure during anesthesia.
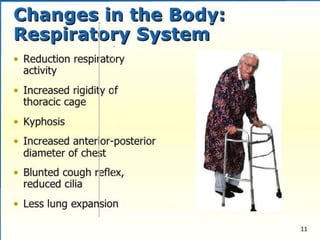
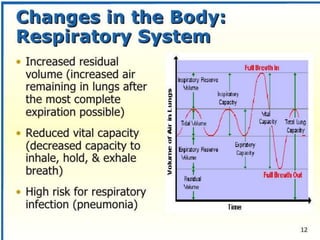
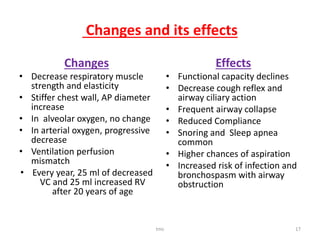
- Respiratory function declines with stiffer lungs and weaker muscles. Elderly are more prone to aspiration, infection, and oxygen desaturation.
- Other organ systems like kidneys, liver and skin also experience changes that slow drug metabolism and clearance. This increases risks of toxicity.
- Thorough



























![Thyroid ppt [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/thyroidpptautosaved-170310134424-thumbnail.jpg?width=640&height=640&fit=bounds)


















































