Pharmacokinetics is the study of the movement of drug molecules in the body. It includes absorption, distribution, metabolism, and excretion of drugs. Pharmacokinetics is the study of what happens to drugs once they enter the body (the movement of the drugs into, within, and out of the body). For a drug to produce its specific response, it should be present in adequate concentrations at the site of action. This depends on various factors apart from the dose.
Four pharmacokinetic properties determine the onset, intensity, and the duration of drug action (Figure 1.6.1):
• Absorption: First, absorption from the site of administration permits entry of the drug (either directly or indirectly) into plasma.
• Distribution: Second, the drug may then reversibly leave the bloodstream and distribute it into the interstitial and intracellular fluids.
• Metabolism: Third, the drug may be biotransformed by metabolism by the liver or other tissues.
• Elimination: Finally, the drug and its metabolites are eliminated from the body in urine, bile, or feces.
In short, pharmacokinetics means what the body does to the drug.
Pharmacokinetics is the study of the movement of drug molecules in the body. It includes absorption, distribution, metabolism, and excretion of drugs. Pharmacokinetics is the study of what happens to drugs once they enter the body (the movement of the drugs into, within, and out of the body). For a drug to produce its specific response, it should be present in adequate concentrations at the site of action. This depends on various factors apart from the dose.
Four pharmacokinetic properties determine the onset, intensity, and the duration of drug action (Figure 1.6.1):
• Absorption: First, absorption from the site of administration permits entry of the drug (either directly or indirectly) into plasma.
• Distribution: Second, the drug may then reversibly leave the bloodstream and distribute it into the interstitial and intracellular fluids.
• Metabolism: Third, the drug may be biotransformed by metabolism by the liver or other tissues.
• Elimination: Finally, the drug and its metabolites are eliminated from the body in urine, bile, or feces.
In short, pharmacokinetics means what the body does to the drug.
For More Medicine Free PPT - http://playnever.blogspot.com/
For Health benefits and medicine videos Subscribe youtube channel - https://www.youtube.com/playlist?list=PLKg-H-sMh9G01zEg4YpndngXODW2bq92w
This presentation will give the students a basic knowledge about the pharmacokinetics of durgs. It will help them clear the basics before digging deep into the topic.
Pharmacodynamics is the study of the biochemical and physiological effects of drugs and their mechanisms of action. Pharmacodynamics is often referred to as “what the drug does to the body”.
In order to exert their effects, drugs usually interact in a structurally specific way with a protein receptor or act on physiological processes within the body. This activates a secondary messenger system that produces a physiological effect. Drugs do not create new action but they can only modify (alter) the functions of cells or tissues in body. The drug–receptor complex initiates alterations in biochemical and/or molecular activity of a cell by a process called signal transduction.
A power point presentation on Pharmacodynamics (what drug does to the body) suitable for undergraduate medical students beginning to study Pharmacology
Review on various families of drug transporters in our body, their functions & drugs acting through them & drug interactions involving these transporters
Presentation covers the basics of pharmacokinetic. Mechanism for the transport of drug molecule. Absorption, factors affecting on absorption of drugs. Concept of bioavailability. Distribution, plasma protein binding, tissue binding, barriers.
For More Medicine Free PPT - http://playnever.blogspot.com/
For Health benefits and medicine videos Subscribe youtube channel - https://www.youtube.com/playlist?list=PLKg-H-sMh9G01zEg4YpndngXODW2bq92w
This presentation will give the students a basic knowledge about the pharmacokinetics of durgs. It will help them clear the basics before digging deep into the topic.
Pharmacodynamics is the study of the biochemical and physiological effects of drugs and their mechanisms of action. Pharmacodynamics is often referred to as “what the drug does to the body”.
In order to exert their effects, drugs usually interact in a structurally specific way with a protein receptor or act on physiological processes within the body. This activates a secondary messenger system that produces a physiological effect. Drugs do not create new action but they can only modify (alter) the functions of cells or tissues in body. The drug–receptor complex initiates alterations in biochemical and/or molecular activity of a cell by a process called signal transduction.
A power point presentation on Pharmacodynamics (what drug does to the body) suitable for undergraduate medical students beginning to study Pharmacology
Review on various families of drug transporters in our body, their functions & drugs acting through them & drug interactions involving these transporters
Presentation covers the basics of pharmacokinetic. Mechanism for the transport of drug molecule. Absorption, factors affecting on absorption of drugs. Concept of bioavailability. Distribution, plasma protein binding, tissue binding, barriers.
The Indian Dental Academy is the Leader in continuing dental education , training dentists in all aspects of dentistry and
offering a wide range of dental certified courses in different formats.
Pharmacokinetics - drug absorption, drug distribution, drug metabolism, drug ...http://neigrihms.gov.in/
A power point presentation on general aspects of Pharmacokinetics suitable for undergraduate medical students beginning to study Pharmacology. Also suitable for Post Graduate students of Pharmacology and Pharmaceutical Sciences.
Couples presenting to the infertility clinic- Do they really have infertility...Sujoy Dasgupta
Dr Sujoy Dasgupta presented the study on "Couples presenting to the infertility clinic- Do they really have infertility? – The unexplored stories of non-consummation" in the 13th Congress of the Asia Pacific Initiative on Reproduction (ASPIRE 2024) at Manila on 24 May, 2024.
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Ve...kevinkariuki227
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journeygreendigital
Tom Selleck, an enduring figure in Hollywood. has captivated audiences for decades with his rugged charm, iconic moustache. and memorable roles in television and film. From his breakout role as Thomas Magnum in Magnum P.I. to his current portrayal of Frank Reagan in Blue Bloods. Selleck's career has spanned over 50 years. But beyond his professional achievements. fans have often been curious about Tom Selleck Health. especially as he has aged in the public eye.
Follow us on: Pinterest
Introduction
Many have been interested in Tom Selleck health. not only because of his enduring presence on screen but also because of the challenges. and lifestyle choices he has faced and made over the years. This article delves into the various aspects of Tom Selleck health. exploring his fitness regimen, diet, mental health. and the challenges he has encountered as he ages. We'll look at how he maintains his well-being. the health issues he has faced, and his approach to ageing .
Early Life and Career
Childhood and Athletic Beginnings
Tom Selleck was born on January 29, 1945, in Detroit, Michigan, and grew up in Sherman Oaks, California. From an early age, he was involved in sports, particularly basketball. which played a significant role in his physical development. His athletic pursuits continued into college. where he attended the University of Southern California (USC) on a basketball scholarship. This early involvement in sports laid a strong foundation for his physical health and disciplined lifestyle.
Transition to Acting
Selleck's transition from an athlete to an actor came with its physical demands. His first significant role in "Magnum P.I." required him to perform various stunts and maintain a fit appearance. This role, which he played from 1980 to 1988. necessitated a rigorous fitness routine to meet the show's demands. setting the stage for his long-term commitment to health and wellness.
Fitness Regimen
Workout Routine
Tom Selleck health and fitness regimen has evolved. adapting to his changing roles and age. During his "Magnum, P.I." days. Selleck's workouts were intense and focused on building and maintaining muscle mass. His routine included weightlifting, cardiovascular exercises. and specific training for the stunts he performed on the show.
Selleck adjusted his fitness routine as he aged to suit his body's needs. Today, his workouts focus on maintaining flexibility, strength, and cardiovascular health. He incorporates low-impact exercises such as swimming, walking, and light weightlifting. This balanced approach helps him stay fit without putting undue strain on his joints and muscles.
Importance of Flexibility and Mobility
In recent years, Selleck has emphasized the importance of flexibility and mobility in his fitness regimen. Understanding the natural decline in muscle mass and joint flexibility with age. he includes stretching and yoga in his routine. These practices help prevent injuries, improve posture, and maintain mobilit
New Drug Discovery and Development .....NEHA GUPTA
The "New Drug Discovery and Development" process involves the identification, design, testing, and manufacturing of novel pharmaceutical compounds with the aim of introducing new and improved treatments for various medical conditions. This comprehensive endeavor encompasses various stages, including target identification, preclinical studies, clinical trials, regulatory approval, and post-market surveillance. It involves multidisciplinary collaboration among scientists, researchers, clinicians, regulatory experts, and pharmaceutical companies to bring innovative therapies to market and address unmet medical needs.
The prostate is an exocrine gland of the male mammalian reproductive system
It is a walnut-sized gland that forms part of the male reproductive system and is located in front of the rectum and just below the urinary bladder
Function is to store and secrete a clear, slightly alkaline fluid that constitutes 10-30% of the volume of the seminal fluid that along with the spermatozoa, constitutes semen
A healthy human prostate measures (4cm-vertical, by 3cm-horizontal, 2cm ant-post ).
It surrounds the urethra just below the urinary bladder. It has anterior, median, posterior and two lateral lobes
It’s work is regulated by androgens which are responsible for male sex characteristics
Generalised disease of the prostate due to hormonal derangement which leads to non malignant enlargement of the gland (increase in the number of epithelial cells and stromal tissue)to cause compression of the urethra leading to symptoms (LUTS
Knee anatomy and clinical tests 2024.pdfvimalpl1234
This includes all relevant anatomy and clinical tests compiled from standard textbooks, Campbell,netter etc..It is comprehensive and best suited for orthopaedicians and orthopaedic residents.
Recomendações da OMS sobre cuidados maternos e neonatais para uma experiência pós-natal positiva.
Em consonância com os ODS – Objetivos do Desenvolvimento Sustentável e a Estratégia Global para a Saúde das Mulheres, Crianças e Adolescentes, e aplicando uma abordagem baseada nos direitos humanos, os esforços de cuidados pós-natais devem expandir-se para além da cobertura e da simples sobrevivência, de modo a incluir cuidados de qualidade.
Estas diretrizes visam melhorar a qualidade dos cuidados pós-natais essenciais e de rotina prestados às mulheres e aos recém-nascidos, com o objetivo final de melhorar a saúde e o bem-estar materno e neonatal.
Uma “experiência pós-natal positiva” é um resultado importante para todas as mulheres que dão à luz e para os seus recém-nascidos, estabelecendo as bases para a melhoria da saúde e do bem-estar a curto e longo prazo. Uma experiência pós-natal positiva é definida como aquela em que as mulheres, pessoas que gestam, os recém-nascidos, os casais, os pais, os cuidadores e as famílias recebem informação consistente, garantia e apoio de profissionais de saúde motivados; e onde um sistema de saúde flexível e com recursos reconheça as necessidades das mulheres e dos bebês e respeite o seu contexto cultural.
Estas diretrizes consolidadas apresentam algumas recomendações novas e já bem fundamentadas sobre cuidados pós-natais de rotina para mulheres e neonatos que recebem cuidados no pós-parto em unidades de saúde ou na comunidade, independentemente dos recursos disponíveis.
É fornecido um conjunto abrangente de recomendações para cuidados durante o período puerperal, com ênfase nos cuidados essenciais que todas as mulheres e recém-nascidos devem receber, e com a devida atenção à qualidade dos cuidados; isto é, a entrega e a experiência do cuidado recebido. Estas diretrizes atualizam e ampliam as recomendações da OMS de 2014 sobre cuidados pós-natais da mãe e do recém-nascido e complementam as atuais diretrizes da OMS sobre a gestão de complicações pós-natais.
O estabelecimento da amamentação e o manejo das principais intercorrências é contemplada.
Recomendamos muito.
Vamos discutir essas recomendações no nosso curso de pós-graduação em Aleitamento no Instituto Ciclos.
Esta publicação só está disponível em inglês até o momento.
Prof. Marcus Renato de Carvalho
www.agostodourado.com
Acute scrotum is a general term referring to an emergency condition affecting the contents or the wall of the scrotum.
There are a number of conditions that present acutely, predominantly with pain and/or swelling
A careful and detailed history and examination, and in some cases, investigations allow differentiation between these diagnoses. A prompt diagnosis is essential as the patient may require urgent surgical intervention
Testicular torsion refers to twisting of the spermatic cord, causing ischaemia of the testicle.
Testicular torsion results from inadequate fixation of the testis to the tunica vaginalis producing ischemia from reduced arterial inflow and venous outflow obstruction.
The prevalence of testicular torsion in adult patients hospitalized with acute scrotal pain is approximately 25 to 50 percent
3. Pharmacokinetics is the quantitative study of
drug movement in, through and out of the body.
Intensity of effect is related to the concentration
of the drug at the site of action, which depends
on its pharmacokinetic properties.
Pharmacokinetic properties of the drug
determine the route(s) of administration, dose,
latency of onset, time of peak action, duration
of action and frequency of drug administration.
7. All pharmacokinetics processes involve transport
of the drug across biological lipid membrane.
Passive diffusion
through lipid
Filtration Carrier transport
8. Passive transport
- Passive diffusion
- Filtration
Specialized transport
- Carrier transport
Active transport
Facilitated diffusion
- Pinocytosis, etc.
Convection
9. Passive (simple) diffusion
The lipid soluble unionized drug diffuse across
the lipid biomembrane in the direction of their
concentration gradient. It does not need energy.
Most drugs are week electrolytes. Their ionization
is pH dependent. The ionization of a week acid (AH)
is given by the equation of Henderson–Hasselbalch:
pKa = pH + log10 ------
[AH]
[A-
]
10. pKa is the negative logarithm of acidic dissociation
constant of the week electrolyte. If the concentration
of unionized drug [AH] is equal to concentration of
ionized drug [A-
], then
[AH]
--------- = 1
[A-
]
since log 1 is 0, under this condition pH = pKa
In this case the molecules of drugs are 50% ionized.
pKb = pH + log10 ------
For a week base:
[BH+
]
[B]
11. Filtration
Filtration is passage of a drug through aqueous pores
in the membrane through paracelullar spaces.
The moving force is hydrostatic or osmotic pressure.
Lipid insoluble drugs cross the biomembrane by
filtration only if their molecular size is smaller than
the diameter of the enlarged aqueous pores.
The filtration has an importance mainly at the level
of renal glomerulus, where the size of capillaries have
large pores (40 Å) and most drugs (even albumin)
can filtrate. The brain capillary pores have small size.
12.
13. Carrier transport –
by combination with a carrier molecule which acts as
a ferry-boat across the lipid region of the membrane.
Carrier transport is saturable and competitively
nhibited by analogues which utilize the same carrier.
a) Active transport is a movement against the con-
centration gradient. It needs energy and is inhibited
by metabolic poisons.
Levodopa and methyldopa are actively absorbed
rom the gut by aromatic amino acid transport.
14. ) Facilitated diffusion. This proceeds more rapidly
han passive (simple) diffusion and translocates
ven nondiffusible substrates, but along their
oncentration gradient, therefore, does not
eed energy. Example: Facilitated transport of glucose.
Pinocytosis involves the invagination of a part
of the cell membrane and trapping within the cell
of a small vesicle containing extracellular consti-
tuents. The vesicle contents can than be released
within the cell, or extruded from the other side of
the cell. Pinocytosis is important for the transport
of some macromolecules (e.g. insulin through BBB).
15. I. ABSORPTIONI. ABSORPTION
It is the passage of drug from the site
of administration into the circulation.
Aqueous solubility. Drugs given in solid form must
dissolve in the aqueous biophase before they are
absorbed. For poorly water soluble drugs (aspirin,
griseofulvin) the rate of dissolution governs the rate
of absorption. If a drug is given as water solution,
it is absorbed faster than the same given in solid
form or as a oily solution.
16. Concentration. Passive transport depends on the
concentration gradient. A drug given as concentrated
solution is absorbed faster than dilute solution.
Area of absorbing surface. If the area is larger,
the absorption is faster.
Vascularity of absorbing surface. Blood circu-
lation removes the drug from the site of absorption
and maintains concentration gradient across the
membrane. Increased blood flow hastens
drug absorption.
17. Route of administration affects drug
absorption, because each route has its
own peculiarities.
Oral application. Unionized lipid soluble drugs (e.g.
ethanol) are readily absorbed from GIT. Acid drugs (aspi-
rin, barbiturates, etc.) are predominantly unionized in the
acid gastric juice and are absorbed from the stomach. Acid
drugs absorption from the stomach is slower, because the
mucosa is thick, covered with mucus and the surface is small.
Basic drugs (e.g. atropine, morphine, etc.) are largely ioni-
zed and are absorbed only from the duodenum.
18. Presence of food dilutes the drug and retards absorption.
Certain drugs form poorly absorbed complexes with food
constituents, e.g. tetracyclines with calcium present in milk.
Food delays gastric emptying.Most drugs are absorbed
better if taken on an empty stomach. Highly ionized drugs,
e.g. amikacin, gentamicin, neostigmine, are poorly
absorbed when given orally.
Certain drugs are degraded in the GIT, e.g. penicillin G
by acid, insulin by peptidases, and are ineffective orally.
Enteric coated tablets (having acid resistant coating) and
sustained released preparations can be used to overcome
acid ability, gastric irritancy and brief duration of action.
20. Drugs can also alter absorption by gut wall effect:
altering motility (atropine, amitriptyline, pethidine,
methoclopramide) or causing mucosal damage
(neomycin, methotrexate, reserpine, vinblastine).
Alteration of gut flora by antibiotics may disrupt the
enterohepatic recirculation of oral contraceptives
and digoxin.
S.c. and i.m. application
By these routes the drug is deposited in the vicinity of
the capillaries. Lipid soluble drugs pass readily across
the whole surface of the capillary endothelium, but
very large molecules are absorbed through lymphatics.
21. Many drugs not absorbed orally are absorbed parenterally.
Absorption from s.c. site is slower than that from i.m. site,
but both are generally faster and more predictable than
p.o. absorption. Application of heat and muscular exercise
accelerate drug absorption by increasing blood flow.
Application of vasoconstrictors (e.g. adrenaline) retard
absorption. Many depot preparations (preparations with a
long action), such as benzatine benzylpenicillin and
protamine zinc insulin can be given by these routes.
Topical applications
(skin, cornea, mucous membranes)
Systemic absorption depends on lipid solubility.
Only a few drugs significantly penetrate intact skin.
22. Nitroglycerine, hyoscine (scopolamine) and estradiol
have been used in this manner. Glucocorticosteroids
(GCS) applied over extensive areas can produce
systemic effects and pituitary-adrenal suppression.
Cornea is permeable to lipid soluble, unionized physo-
stigmine but not to highly ionized neostigmine.
Similarly, the mucous membrane of the mouth,
rectum and vagina absorb lipophilic drugs, e.g.
estrogen cream applied intravaginally has produced
gynecomastia in the male partner.
23. Bioavailability refers to the rate and extent of
absorption of a drug from dosage form as determined
by its concentration-time curve in blood or by its excretion
n urine. It is a measure of the fraction (F) of administered
dose of a drug that reaches the systemic circulation in the
unchanged form.
Bioavailability of a drug injected i.v. is 100%, but is
requently lower after oral ingestion, because:
a) The drug may incompetely absorb
b) The absorbed drug may undergo first pass
metabolism in intestinal wall and/or liver, or be
excreted in bile.
24. Time (h)
10 1550
(i.v. application)
(p.o. application)
Plasmaconcentration(mcg/ml)
AUC p.o.
F = ------------ x 100%
AUC i.v.
AUC – area under the curve
F – bioavailability
25. Plasma concentration time curves of the three preparations of a drug
which contain the same amount. Formulation B is more slowly absorbed
than A and may not produce therapeutic effect. Formulation C is absorbed
to a lesser extent (it has lower bioavailability).
26. II. DISTRIBUTIONII. DISTRIBUTION
In studying the pharmacokinetics biosystems
conditionally divided into separate parts –
compartment (or phases).
They are virtual spaces in which the drug
is evenly distributed. They are distinguished
each other in the volume of distribution
and invasion (penetration) and
evazionnite (release) rate constants.
27. The distribution of the drugs is a dynamic process,
during which they pass from the central (plasma)
compartment in the tissue to reach steady state
(steady state – ss). It depends on the mode of
administration and the pK of the drug, its ability
for binding to plasma protein, pH of the medium,
organ perfusion.
The number of compartments is determined for
each drug according to the experimental data
measured concentrations at different moments
in the blood, urine and body fluids.
29. Body fluid compartments
The total body water as a percentage of body
mass varies from 50% to 70%, being rather
less in women than in man.
Body water is distributed
into the following main compartments:
1. plasma (5% of body mass)
2. intestinal fluid (16%)
3. intracellular fluid (35%)
4. transcellular fluid (2%)
5. fat (20%)
30. Apparent volume of distribution (Vd)
It is accept that the body behaves as a single
homogeneous compartment with volume (Vd)
in which the drug gets immediately distributed:
Vd = -----------------------------
Dose administered
Plasma concentration
31. Drugs extensively bound to plasma proteins are largely
restricted to the vascular compartment and have low Vd
(e.g. warfarin – 99% bound and its Vd is 0,1 L/kg).
Drugs sequestrated in other tissues may have Vd much
more than the total body water or even body mass, e.g.
digoxin (6 L/kg) and propranolol (3 to 4 L/kg) because
most of the drug is present in other tissues, and the
plasma concentration is low.
Therefore, in case of poisoning, drugs with large
Vd are not easily removed by haemodialysis.
32. Redistribution. Highly lipid soluble drugs given i.v.
or by inhalation get distributed to organs with high
blood flow (brain, heart, kidney, liver). Later they get
distributed to less vascular tissues (muscles and fat)
and the drug-plasma concentrations falls.
The greater lipid solubility of the drug hastens its
redistribution. Anaesthetic action of thiopentone
(thiopental) is terminated in few minutes due to
redistribution. However, when the same drug is given
repeatedly or continuously over long periods the low
perfusion high capacity sites get progressively filled
up and the drug becomes longer acting.
34. Blood brain barrier (BBB): includes the capillary en-
dothelial cells (which have tight junctions and lack large
intracellular pores) and an investment of glial tissue,
over the capillaries. A similar barrier is loctated in
the choroid plexus.
35. BBB is lipid and limits the entry of non-lipid soluble
drugs (amikacin, gentamicin, neostigmine etc.).
Only lipid soluble unionized drugs penetrate and
have action on the CNS.
Efflux carriers like P-gp (glycoprotein) present in brain
capillary endothelial cells (also in intestinal mucosal,
renal tubular, hepatic canicular, placental, and testicular
cells) extrude drugs that enter the brain by other processes.
Inflammation of the meninges of the brain increases
permeability of the BBB.
Dopamine (DA) does not enter the brain, but its precursor
levodopa does. This is used later in parkinsonism.
37. Placental barrier. Placental membranes are lipid
and allow free passage of lipophilic drug, while restricting
hydrophilic drugs. The placental P-gp also serves to
limit foetal exposure to maternally administered drugs.
However restricted amounts of nonlipid soluble drugs,
when present in high concentration or for long periods
in maternal circulation, gain access to the foetus. Thus, it
is an incomplete barrier and many drugs, taken by the
mother, can affect the foetus or the newborn.
Penicillins, azithromycin, and erythromycin do not affect
the foetus and can be used during the pregnancy.
38. Plasma protein binding (PPB). Most drugs possess
hysicochemical affinity for plasma proteins. Acidic
drugs bind to plasma albumin and basic drugs
o α1-glycoprotein. Extent of binding depends on the in-
ividual compound. Increasing the concentration of a drug
an progressively saturate the binding sites. The clinical
ignificant implications of PPB are:
) Highly PPB drugs are largely restricted to the vascular
compartment and tend to have lower Vd.
) The PPB fraction is not available for action.
) There is an equilibration between the PPB fraction of
the drug and the free molecules of the drug.
39. d) The drugs with high physicochemical affinity for
plasma proteins (e.g. aspirin, sulfonamides,
chloramphenicol) can replace the other drugs
(e.g. acenocoumarol, warfarin) or endogenous
compounds (bilirubin) with lower affinity.
e) High degree of protein binding makes the drug long-
acting, because bound fraction is not available for
metabolism, unless it is actively excreted by the liver
or kidney tubules.
f) Generally expressed plasma concentrations of the drug
refer to bound as well as free drug.
g) In hypoalbuminemia, binding may be reduced and high
concentration of free drug may be attained (e.g. phenytoin).
40. Tissue storage. Drugs may also accumulate in specific
organs or get bound to specific tissue constituents, e.g.:
Heart and skeletal muscles – digoxin (to muscle proteins)
Liver – chloroquine, tetracyclines, digoxin
Kidney – digoxin, chloroquine
Thyroid gland – iodine
Brain – chlorpromazine, isoniazid, acetazolamide
Retina – chloroquine (to nucleoproteins)
Iris – ephedrine, atropine (to melanin)
Bones and teeth – tetracyclines, heavy metals
(to mucopolysaccharide of connective tissue)
Adipose tissues – thiopental, ether, minocycline, DDT
41. III. METABOLISM (BIOTRANSFORMATION)III. METABOLISM (BIOTRANSFORMATION)
Metabolism includes chemical alteration of the drugs in
he body. Most hydrophilic drugs (amikacin, gentamycin,
neostigmine, mannitol) are not biotransformated and are
excreted unchanged. The mechanism to metabolize drugs
s developed to protect the body from toxins. The primary
site for drug metabolism is the liver, other sites are the
kidney, intestine, lungs, and plasma.
Metabolism of drugs may lead to the following:
a) Inactivation. Most drugs and their active metabolites
are converted to less active or inactive metabolites, e.g.
phenobarbital, morphine, propranolol, etc.
42. b) Active metabolite from an active drug. Many drugs
are converted to one or more active metabolites (e.g.
diazepam, amitriptyline).
c) Activation of inactive drug. Few drugs (so called
prodrugs) are inactive as such. They need conversion
in the body to one or more active metabolites (e.g.
levodopa, benfothiamine, enalapril, perindopril).
The prodrug may offer advantages: their active forms
may be more stable; they can have better bioavailability
(e.g. benfothiamine), or other desirable
pharmacokinetic properties or less
side effects and toxicity.
43. Biotransformation reactions can be classified into two
phases: I (no synthetic) and II (synthetic, conjugation).
Phase I (no synthetic reactions)
a) Oxidation is the most important drug metabolizing
reaction. Various oxidation reactions are hydroxylation;
oxygenation at C-, N- or S-atoms; N or 0-dealkylation,
oxidative deamination, etc. Oxidative reactions are
mostly carried out by a group of monooxygenases in
the liver, which in the final step involve cytochrome P450
reductase and O2. There are more than 200 cytochrome
P450 isoenzymes, differing in their affinity for various
substances (drugs). They are grouped into > 20 families.
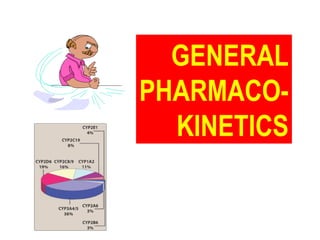
44. CYP 3A4/5 carry out biotransforma-
tion of the largest number (≈ 50%) of
drugs. In addition to the liver, these isoforms
are expressed in the intestine (responsible for first pass
metabolism at this site) and the kidney too. Inhibition of
CYP 3A4 by erythromycin, clarithromycin, ketoconzole,
itraconazole, verapamil, diltiazem, and a constituent of
grape fruit juice are responsible for unwanted interaction
with terfenadine. Rifampicin, phenytoin, carbmazepine,
phenobarbital are inducers of the CYP 3A4.
46. Barbiturates, phenothiazines, paracetamol, streroids,
phenytoin, benzodiazepines, theophyllin and many other
drugs are oxydaized by CYP450. Some other drugs
(adrenaline, mercaptopurine) and ethanol are oxidized
by mitochondrial or cytoplasmic enzymes.
47. b) Reduction. This reaction is conversed
of oxidation and involves CYP450 enzymes
working in the opposite direction.
Drugs, primarily reduced, are
chloramphenicol, halothane.
48. Ester + H20 Acid + Alcohol
Esterase
Similarly amides and polypeptides are hydrolyzed
by amidase and peptidases. Hydrolysis occurs in the liver,
intestines, plasma, and other tissues. Examples are
choline esters, procaine, lidocaine, pethidine, oxytocin.
d) Cyclization is formation of a ring structure from a
straight chain compound, e.g. proguanil.
e) Decyclization is opening up of a ring structure of
the cyclic molecule, e.g. phenytoin, barbiturates.
c) Hydrolysis. This is cleavage of a drug molecule by
taking up a molecule of water.
49. Phase II – synthetic (conjugation) reactions
These involve conjugation of the drug or its phase I meta-
bolite with an endogenous substrate to form a polar highly
ionized organic acid, which is easily excreted in urine or
bile. Conjugation reactions have high energy requirements.
(1) Glucoronide conjugation is the most important syn-
thetic reaction. Compounds with a hydroxyl or carboxylic
acid group are easily conjugated with glucuronic acid,
which is derived from glucose, e.g. chloramphenicol,
aspirin, morphine, metronidazole, GCS, bilirubin, thyroxine.
Drug glucuronides, excreted in bile, can be hydrolyzed
in the gut by bacteria, producing beta-glucuronidase.
50. The liberated drug is reabsorbed and undergoes the same
fate. This enterohepatic recirculation of some drugs (e.g.
chloramphenicol, phenolphthalein, oral contraceptives)
prolongs their action.
(2) Acetylation. Compounds having amino or hydrazine
residues are conjugated with the help of acetyl CoA, e.g.
sulfonamides, isoniazid. Multiple genes control the acetyl
transferases and rate of acetylation shows genetic
polymorphism (slow and fast acetylators).
(3) Sulfate conjugation. The phenolic compounds and
steroids are sulfated by sulfokinases, e.g.
chloramphenicol, adrenal, and sex steroids.
53. (4) Methylation. The amines and phenols can be
methylated. Methionine and cysteine act as methyl donors.
Examples: adrenaline, histamine, nicotinic acid.
(5) Ribonucleoside/nucleotide synthesis is important
for the activation of many purine and pyrimidine antimeta-
bolites used in cancer chemotherapy, e.g. Xeloda®
.
(6) Only a few drugs are metabolized by enzymes of
intermediary metabolism. Examples:
•alcohol by dehydrogenases
•allopurinol by xanthine oxidase
•succinylcholine and procaine by plasma cholinesterase
•adrenaline by monoamine oxidase (MAO)
54. FIRST PASS (PRESYSTEMIC) METABOLISM
This refers to metabolism of a drug during its passage
from the site of absorption into systemic circulation. All
orally administered drugs are exposed to drug metabo-
lism in the intestinal wall and liver in different extent.
•High first pass metabolism: propranolol, verapamil,
pethidine, salbutamol, nitroglycerine, morphine, lidocaine.
•Oral dose of these drugs is higher than sublingual or
parenteral dose.
•There is individual variation in the oral dose due to
differences in the extent of first pass metabolism.
•Oral bioavailability is increased in patients with severe
liver disease.
55. IV. EXCRETIONIV. EXCRETION
Excretion is the passage out of
systematically absorbed drugs.
Drugs and their metabolites
are excreted in:
urine (through the kidney)
•bile and faeces
•exhaled air
•saliva and sweat
•milk
•skin
56. The kidney is responsible for excreting all
water soluble substances.
Glomerular filtration. Glomerular capillaries have large
pores. All nonprotein bound drugs (lipid soluble or insoluble)
presented to the glomerulus are filtrated. Glomerular filtration
of drugs depends on their plasma protein binding and renal
blood flow. Glomerular filtration rate (g.f.r.) declines
progressively after the age of 50 and is low in renal failure.
Tubular reabsorption. Lipid soluble drugs filtrated at the
glomerulus back diffuse in the tubules because 99% of
glomerular filtrate is reabsorbed, but nonlipid soluble
and highly ionized drugs are unable to do so.
57. Thus, the rate of excretion of such drugs, e.g.
aminoglycoside (amikacin, gentamicin, tobramycin) parallels
g.f.r. Changes in urinary pH affect tubular reabsorption of
partially ionized drugs:
•Weak bases ionize more and are less reabsorbed
in acidic urine.
•Weak acids ionize more and are less reabsorbed
in alkaline urine.
This principle is utilized for facilitating elimination
of drugs in poisoning:
•Urine is acidified in morphine and atropine poisoning.
•Urine is alkalized in barbiturate and salicylate poisoning.
58. The effect of changes in urinary pH on drug excretion
is greatest for a drug having pK values between 5 to 8,
because only in this case pH dependent passive
reabsorption is significant.
Tubular secretion is the active transfer of organic acid
and bases by two separate nonspecific mechanisms,
which operate in the proximal tubules:
•Organic acid transport for penicillins, probenecid,
salicylates, uric acid, sulfinpyrazones, nitrofurantoin,
methotrexate, drug glucuronides, etc.
•Organic base transport for thiazides, quinine,
procainamide, cimetidine, amiloride, etc.
59. Many drug interactions occur due to competition
for tubular excretion, e.g.:
•Aspirin blocks uricosuric action of probenecid and sulfin-
pyrazone and decreases tubular excretion of methotrexate.
•Probenecide decreases the urine concentration of
nitrofurantoin, increases the duration of penicillin action
and impairs excretion of methotrexate.
•Quinidine decreases renal and biliary clearance of digoxin
by inhibiting efflux carrier P-gp.
Tubular transport mechanisms are not well developed
at birth. Duration of action of many drugs (penicillins,
cephalospoins, aspirin, etc.) is longer in neonates.
These systems mature during infancy.
66. KINETICS OF ELIMINATION
(elimination = metabolism + excretion)
Clearance (Cl) of a drug is the theoretical volume of plasma
from which the drug is completely removed per unit time:
Cl = Rate of elimination/Plasma concentration
Renal (Clr) or creatinine clearance (Clcr):
Clrenal = --------------------
Cplasma
Curine x Vurine
67. First order (exponential) kinetics. For majority of drugs
the processes involved in elimination are not saturated
over the clinically obtained concentrations. These drugs
have first order kinetics. Their rate of elimination is
directly proportional to plasma drug concentration and
their clearance
remains constant.
69. Zero order (linear) kinetics.
In a few cases where the drugs are inactivated
by metabolic degradation (such as ethanol,
phenytoin, theophylline, salicylates, and warfarin),
the time-course of disappearance of the drug from
the plasma does not follow the exponential or
biexponential pattern, but is initially linear.
These drugs are removed at a constant rate
which is independent of plasma concentration.
This is often called zero order kinetics.
71. Plasma half live (t1/2) is the time in which the plasma
concentration of a drug declines by one half. Drug with
long t1/2 can accumulate. Plasma t1/2 of some drugs:
Adenosine < 2 sec
Dobutamine – 2 min
Benzylpenicillin – 30 min
Amoxicillin – 1 h
Paracetamol – 2 h
Atenolol – 7 h
Diazepam – 40 h
Ethosuccimide – 54 h
Digitoxin – 168 h
72. From the peak plasma concentration the drug is vir-
tually eliminated from the plasma in 5 t1/2 periods:
(1) (2) (3) (4) (5)