Downloaded 97 times



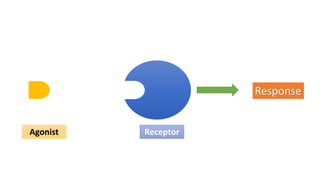
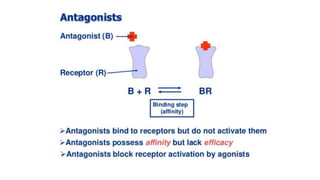


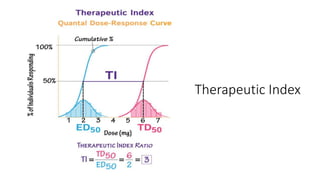

La farmacodinamia estudia los efectos bioquímicos y fisiológicos de los medicamentos y sus mecanismos de acción, interactuando de manera específica con los receptores proteicos del cuerpo. Las drogas pueden aumentar o disminuir la actividad celular, además de tener efectos de irritación, acción química o acción citotóxica, dependiendo del tipo de receptor y la interacción con otros medicamentos. Se destaca la importancia del índice terapéutico para medir la seguridad de un fármaco, diferenciando entre dosis efectivas y tóxicas.




































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





