Pharmacokinetics /prosthodontic courses
•
2 likes•906 views

The Indian Dental Academy is the Leader in continuing dental education , training dentists in all aspects of dentistry and offering a wide range of dental certified courses in different formats.

More Related Content
What's hot
What's hot (20)
Viewers also liked
Similar to Pharmacokinetics /prosthodontic courses
Similar to Pharmacokinetics /prosthodontic courses (20)
More from Indian dental academy
More from Indian dental academy (20)
Recently uploaded
Recently uploaded (20)
Pharmacokinetics /prosthodontic courses
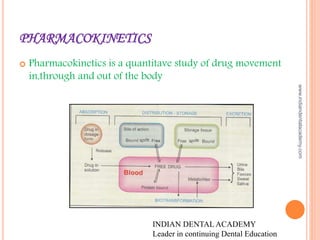
- 1. PHARMACOKINETICS Pharmacokinetics is a quantitave study of drug movement in,through and out of the body INDIAN DENTAL ACADEMY Leader in continuing Dental Education www.indiandentalacademy.com
- 2. Pharmocokinetics include Transport of the across the membrane Absorpiton of the drug Distribution of drug Biotranformation or metabolism of drug Excretion of the drug www.indiandentalacademy.com
- 3. MEMBRANE TRANSPORT Biologic membrane is a bilayer of phospholipids and cholestrol molecules www.indiandentalacademy.com
- 4. DRUGS ARE TRANSPORTED ACROSS THE MEMBRANES BY Passive diffusion and filtration Specilized transport Passive diffusion : The drug Diffuses across the membrane in the direction of its conc. gradient, the membrane playing no active role in the process. It is the most important mechanism for majority of the drugs Lipid soluble drugs diffuse by dissolving in the Lipoidal matrix of the membrane, the rate of transport Being proportional to the lipid: water partition coefficient of the drug A lipid soluble drug attains higher conc. in the membrane and diffuses quickly Also , greater the difference in the conc. of the drug on the two sides of the membrane, faster is the diffusion. www.indiandentalacademy.com
- 5. INFLUENCE OF PH Weakly acidic drugs, which forms salts with cations ionize more at alkaline ph Eg: sodium phenobarbitone,pottasium pencillin v Weakly basic drugs,which forms salts with anions ionize more at acidic ph Eg: atrophine sulphate www.indiandentalacademy.com
- 6. FILTRATION Filtration is the passage of drugs through the acqueous pores in the membrane or through paracellular spaces This can be accelerated if hydrodynamic flow of the solvent is occuring under hydrostatic or osmotic pressure gradient www.indiandentalacademy.com
- 8. CARRIER TRANSPORT : all cell membranes express a host of transmembrane proteins which serve as carrier or transporters for physiologically important ions , neutrients , metabolitestransmitters etc across the membrane Carrier transport is specific for substrate ,saturable, competitively inhibited, analogues which utilizes the same transporter, and is much slower than flux through channels Depending on requirement of energy ,carrier transport is two types Facilitated diffusion Active transport www.indiandentalacademy.com
- 9. FACILITATED DIFFUSION The transporter belonging to the super family of solute carreier(slc) transporters, operates passively without needing energy and translocates the substrates in the direction of its electrochemical gradient that is from higher to lower concenteration It mearly facilitates permeation of a poorly diffusable substrate Eg: the entry of glucose into the muscle and fat cells by Gut www.indiandentalacademy.com
- 10. ACTIVE TRANSPORT It requires energy , is inhibited by metabolic poisons, and transport the solute against its electrochemical gradient i.e low to higher conc , resulting in selective accumulation of the substance on one side of the membrane Active transport can be primary or secondary depending on the sourse of the driving force Primary active transport: energry is obtained diretcly by the hydrolosis of atp The transportrs belong to the super family of atp binding cassete (abc) transpoters whose intracelluar loops have atpase activity they mediate only afflux of the solute from the cytoplasm eighter to ecf or into an intracellular organelle www.indiandentalacademy.com
- 11. Secondary active transport: In this type of active transport effected by another set of SLC transporters, the energy to pump one solute is derived from the down hill movement of another solute (mostly NA) . www.indiandentalacademy.com
- 12. ABSORPTION It is the movement of drug from its site of administration into the circulation Not only the fraction of administered dose that gets absorbed,but also the rate of absorption is also important Except when given i.v ,the drug has to cross bilogical membrane ;absorption is governed by the above described principles.other factors affecting absorption are acqueos solubility , the concentration.area of absorbing surface ,vascularity of the absorbing surface ,route of administration www.indiandentalacademy.com
- 13. BIOAVAILABILITY Bioavailabilty refers to the rate and extent of absorption of drug from a dosage form as determined by its conc –time curve in blood or by its excretion in urine. www.indiandentalacademy.com
- 14. It is a measure of the fraction F of administered dose of a drug that reaches the systemic cirulation in the unchanged form Bioavailability of drug injected Iv is 100%, but is frequently lowered as per oral injesion because a) The drug may be incompletely absorbed b) the absorbed drug may undergo first pass metabolism , in the intestinal wall or liver or the excreted in bile. Incomplete bioavaiability after sc or im injection is less common ,but may occur due to local binding of the drug Differences in bioavailability may arise due to variations in disintegration and dissolution rate . Differences in bioavalabilty are mostly seen with poorly soluble and slowly absorbed drug . www.indiandentalacademy.com
- 15. DISTRIBUTION Once a drug has gained access to the blood stream , its gets distributed to other tissues that initially had no drug , concentration gradient is in the direction of plasma-tissues The extent of distibution of a drug depends on its lipid solubility , ionisation at physiologic ph( a function of its pka ), extend of binding to plasama and tissue proteins, presence of tissue specific transporters and differences in the region of blood flow Movement of a drug proceeds untill an equilibrium is established between unbound drug in plasma and tissue fluids subsequently, there is parallel decline in both due to elimination www.indiandentalacademy.com
- 16. APPARENT VOLUME OF DISTRIBUTION The volume that would accommodate all the drug in the body ,is the conc through out was the same ,as in plasma. Thus it describes the maount of drug present in the body as a multiple of that contained in a unit volume of plasma. www.indiandentalacademy.com
- 17. REDISTRIBUTION Highly lipid soluble drugs gets intilayy distributed to organs with high bolld flow i.e brain heart kidney etc.;later, less vascular but more bulky tissues (muscle,fat) take up the drug –plasma conc falls and the drug is withdrawn from these sites If the site of action of the drug was in one of the highly perfused organs, redistribution results in termination of drug action. Greater the lipid solubility of the drug , faster is its redistribuiton Anastetic action of thiopentene sodium injected I.V isdominated in few minutes due to redistribution www.indiandentalacademy.com
- 18. PENETRATION INTO BRAIN AND CSF www.indiandentalacademy.com
- 19. PLASMA PROTEIN BINDING Most drugs posesses physicochemical affinity for plasma proteins Acidic drugs generally bind to plasma albumin Basic drugs to alpha 1 acid glycoprotein. Binding to albumin is quantitaively importanat Higly plasmaprotein bound drugs are largely restricted to the vascular compartment because the protein bound drug doesnot cross the membrane they tend to have smaller volumes of distribution www.indiandentalacademy.com
- 20. The bound fraction is not available for action however ,it is a equlibrium with a fee drug in plasma and dissociates when the conc of the late r is reduced due to elimination plasma protein binding thus tantamounts to the temporary storage of the drug . HIGH DEGREE OF PROTEIN BINDING generally makes the drug long acting because bound fraction is not available for metabolism or excretion, unless it is actvely extracted in the liver or kidney tubules Generally expressed plasma concentration of the drug refer to ound as well as free drug One drug can bind to may sites on the albumin molecule. Conversly, more than one drug can bind to same site this can give rise to displacement interactions among drugs bound to the same site. Eg: salicylates displace sulfonyl urea www.indiandentalacademy.com
- 21. BIOTRANSFORMATION Biotranspformation means chemical alteration of the drug in the body It is needed to render nonpolar(lipid soluble) compounds polar(lipid insoluble) so that there are not reabsorbed in the renal tubules and are excreted . Most hydrophillic drugs eg: strptomycin are little biotransformed they are largely excreted unchanged Mechanisms which metabolise drugs( essentially foregin substances ) have developed to protect body from injested toxins Primary site for drug metabolism is liver others are kidneys,intestines,plasma www.indiandentalacademy.com
- 22. Biotransformation of drugs leads to following : A) Inactivation B) Active metabolite from inactive drug C) Activation of inactive drug Inactivation: most drugs ad their active metabolite are rendered inactive or less active eg: ibuprofen,PCT,lidocaine Active metabolite form inactive drug:many drugs have been found to be partially converted to one or more active metabolite www.indiandentalacademy.com
- 23. Activation of inactive drug: few drugs are inactive as such and need conversion in the body in one or more active metabolites such a drug is called prodrug .prodrug may offer advantages over the active form in being more stable , having better bioavailability less side effects and toxicity www.indiandentalacademy.com
- 24. Biotransoformation reaction can be classified into non synthetic or phase 1 or function alization reactions Metabolite may be actve or inactive . Oxidation Reduction Hydrolysis Cyclization Decyclization www.indiandentalacademy.com
- 25. Synthetic or phase 2 reaction : Metabolite is mostly inactive Glucuronide conjugation Acetylation Methylation Sulfate conjugation Glycine conjugation Glutathione conjugation Libonucleoside or nulceotide snthesis www.indiandentalacademy.com
- 26. INHIBITION OF DRUG METABOLISM one drug can competetively inhibit metabolism of another if it utilizes the same enzyme or cofactor www.indiandentalacademy.com
- 27. CON SEQUENCES MICROSOMAL ENZYME INDUCTION Decreased intensity and or duration of action of drugs that are inactivated by metabolism Eg: failure of contraception with oral contraceptives Increased intensity of action of drugs that are activated by metabolism acute PCT toxicity is due to one of its metabolites –toxicity occurs at lower dosage in patients receing enzyme inducers Intermittent use of an inducer may interfere with the adjustment of those of another drug prescribed on regular bases eg: oral anticoagulants ,oral hypoglycemics ,anti epileptics and anti hypertensives www.indiandentalacademy.com
- 28. POSSIBLE USES OF ENZYME INDUCTION Congenital non hemolytic jaundice it is due to deficinet glucoridation of bilurubin ; phenobarbitone hastens cleareance of jaundice Cushings syndrome phenatoin may reduce the manifestation sof enhancing the degradation of adrenosteroids Chronic poisoinings by faster metabolism of the accumulated poisonous substance Liver disease www.indiandentalacademy.com
- 29. FIRST PASS (PRESYSTAMIC) METABOLISM This refers to metabolism of a drug during its passage from the site of absortion into the systemic circulation All orally administerd drugs are exposed to drug metabolizing enzymes in the intestina wall and liver( where they first reach through portal vein) The extent of first pass metabolism differs for different drus and is important for determinant of oral bioavailabilty www.indiandentalacademy.com
- 30. Attributes of drugs with hisg first pass metabolism A) oral dosage cosiderably higher than sub lingual or parenteral dose B) there is marked individual varation in the oral dose due to differences in the xtents of first pass metabolism C)oral bioavailabiltity is apparently increased in patients with severe liver diseases D) oral bioavailability of a drug is increased if another drug competeing with it in first pass metabolism is given concurrently Eg: chlorpromazine and propanalol www.indiandentalacademy.com
- 31. EXCRETION Excretion is the passage out of systemically absorbed drugs Drugs and their metabolites are excreted in Urine Feaces Exhaled air Saliva and sweat Milk www.indiandentalacademy.com
- 32. RENAL EXCRETION Net renal excretion = (glomerular filtration +tubular secretion)- tubular reabsorption Weak bases ionise more and are less reabsorbed in acidic urine Weak acids ionise more and less reabsorbed in alkaline urine Drugs utilizing the same active transport comete with each other Eg: probencid an organic acid which has high affinity for the tubular oatp it blocks the active transport of both pencillin and uric acid Many dug interaction occur due to competetion ofr tubular secretion Salicylates block uricosuric action of probencid And sulfinperazone and decrease tubular secretion of methotrexate www.indiandentalacademy.com
- 33. KINETICS OF ELIMINATION They are 3 fundamental formacokinetics parameters namely Bioavailability(F) Volume of distribution(v) Cleareance (Cl) Drug elimiation is the sumtotal of metabolic inactivation and excretion Drug is eliminated only from the central compartment (blood) which is in equlibrium with perepheral compartments including the site of action www.indiandentalacademy.com
- 34. Depending upon the ability of the body to elimianate a drug, is again the fraction of the central compartment may be considered to be totally “cleared” of that drug in a given period of time to account for elimination over that period www.indiandentalacademy.com
- 35. CLEREANCE Clereance of a drug in the theoritical volume of plasma from which the drug is ocmpletey removed in a unit time It can be caluclated as cl=rate of elimiation /C WHERE C IS THE PLASMA CONC. FOR MAJORITY OF DRUGS THE PREOCESS INVOLVED IN ELIMINIATION ARE NOT SATURATED OVER THE CLINICALLY OBTAINED CONCENTRATIONS www.indiandentalacademy.com
- 36. First order (exponential )kinetics: The rate of elimitation is directly proportional to drug concentraton,CL remains constant Zero order kinetics:The rate of elimination remains constant irrespective of drug concentration ,CL decreases with increase in concentration plasma half-life: The plasma half life (t1/2) of a drug is the time taken for its plasma concentration to be reduced to half of its original value www.indiandentalacademy.com
- 37. PHARMOCOCKINETICS OF NSAID Aspirin: it is absorbed from stomach and small intestine its poor water solubility is a limiting factor in absoorption . Microfining the drug particles and inclusion of an alkali enhances absorption Aspirin is readily deacytylated in gut wall ,liver plasma,and other tiuuses to release salycylic acid which is a major circulating and active form It is 80% bound to plasma protein and has a volume of distribution 0.17 lit/kg It slowly enters the brain but freely crosses plaacenta www.indiandentalacademy.com
- 38. ASPIRIN CONT’D Both aspirin and salycylic acid are conjugated in liver by glycine to give salicyluric acid (major part) and with glucorinic acid. Few other metabolites are also formed Excretion : the metabolites are excreted by GF as well as tubular secretion normally only 1/10th is excreted as free salycylic acid ,it can be increased by alkalysation Plasma half life of aspirin as such is 50-20min , but taken together with that of released salycylic acid it is 3- 5 hrs www.indiandentalacademy.com
- 39. IBUPROFEN It is absorbed orally Higly bound to plasma proteins ( 90-99%), but displacement interactions are not clinically significant- dose of anticoagulants and oral hypoglycemics need not to be altered becoz they inhibit platelet function , use with anticoagulants should, neverthless, be avoided. All propionic acid derivitives enters brain ,synovial fluid and cross placenta They are largely metabolized in liver by hydroxylation and glucuronide conjugation and excreted in urine as well as bile www.indiandentalacademy.com
- 40. DICLOFENAC SODIUM It is well absorbed orally ,99% protein bound, metabolised and excreted both in urine and bile Plasma life is approximately 2hrs however, it had good tissue penetrability and conc in synovial fluid is maintaianed for 3 times longer period than in plasma, exerting extended herpatic action in joints www.indiandentalacademy.com
- 41. KETOROLAC It is rapidly absorbed oral & im administration It is higly plasma protein bound and 60% excreted unchanged in urine. Major metabolic pathway is glucorodination Plasma half life 5- 7hrs www.indiandentalacademy.com
- 42. NIMUSULIDE It is almost completely absorbed orally 99% plasma protein bound Extensively metabolised and excreted mainly in urine 2-5 hrs plasma half life www.indiandentalacademy.com
- 43. PARACETMOL Dethylated active metaboite of phenacetin It is well absorbed orally, only about ¼th is proein bound in plasma and it is uniforamly distributed in the body Metabolism occurs mainly by conjugation with glucuronic acid and sulphate Conjugates are rapidly excreted in urine Plasma half is 2-3 hrs Effect after an oral dose lasts for 3- 5 hrs www.indiandentalacademy.com
- 44. INSULIN Insulin is distributed only extracellularly It is a peptide, gets degraded in git given orally In injected insulin or that released from pancrease is metabolised primarly in liver and to a smaller extent in kidney and muscles Nearly half of the insulin entering portal vein from pancrease is inactivated in the first passage through liver thus normally liver is exposed to much higher conc of insulin than other tissues www.indiandentalacademy.com
- 45. During biotransformation the disulphide bonds are reduced – A n B chains are seperated.these are further broken down to the constituent amino acids Plasma half life 5- 9 mins www.indiandentalacademy.com
- 46. PHENATOIN Absoprtion of phenotoin by oral route is slow mainly because of its poorly acqueous solubility 80-90% bound to plasma protein Widely distribute in the body Metabolised in liver by glucoridination conjugation only 5% unchanged pheotoin is excreted in urine Plasma life is 12- 24 hrs www.indiandentalacademy.com
- 47. CARBAMAZEPINE Oral absorption of c is slow and variable because of poor water solubility It is 75 % bound to plasma protein It is meabolised in liver by oxidation to an active metabolite (10-11 ipoxycarbazepine) as well as by hydroxylation and conjugation to inactive ones It s a substrate as well as inducer of CYP3A4 and other drug metabolizing enzyme Initially its plasma half life is 20 -40 hrs , but, decreases to 10 to 20 hrs on chronic medication due to autoinduction of metabolism www.indiandentalacademy.com
- 48. PHARMOCOKINETICS OF ANTIBIOTICS Ciprofloxacin: it is rapidly absorbed orally but food delays absorption and first pass metabolism occurs The most prominent featue of ciprofloxacin is high tissue pennetrability ,conc in lung ,sputum,muscle , bone, prostrate and phagocytes Exceeds that of plasma, csf and acqueous levels are lowered . It is excreted primarly in urine both by glomerular filtration and tubular secretion Urinary and biliary conc are 10-50 fold higher than plasma www.indiandentalacademy.com
- 49. OFLOXACIN It is relatively lipid soluble Oral bioavailability is high Attains high plasma conc. Food doesnot interfere with its absorption It is excreted largely unchanged in urine Dose needs to be reduced in renal failure www.indiandentalacademy.com
- 50. PENCILLIN G PENCILLIN G IS acid labile destroyed by gastric acid as such less than 1/3rd of an oral dose is absorbed in the active form Absorption of sod.P.g from im site is rapid and complete Peak plasma level is attained in 30 min It is distributed mainly extracellularly Reaches most body fluids, but penetration in serous cavities and csf is poor 60% plasma protein bound It is little metabolised due to rapid excretion The pharmacokinetics of PmG is dominated by very rapid renal excretion; about 105 by glomerular filteration and the rest by tubular secretion www.indiandentalacademy.com
- 51. Plasma half life of pencillin g is 30min in healthy adults Neonates have slower tubular secretion – plasma half life is longer ;but appraches adult value by 3months and its even shorter in childhood Aged and those with renal failure excrete pencillin slowly Tubular secretion of penG CAN be blocked by probencid – higher and longer lasting plasma conc are achieved Probencid also decreases the volume of distribution of pencillins www.indiandentalacademy.com
- 52. AMPICILLIN Ampicillin is not degraded by gastric acid Oral absorption is incompete but adequate Food interferes with absorption It is parly exctreted in bile and reabsorbed- enterohepatic cirulation occurs However,primary zone of excretion is kidney. But tubular secretion is slower than png Plasma half life 1hr www.indiandentalacademy.com
- 53. AMOXCILIN It is a close congener of ampicillin (but not a prodrug);similar to it in all respects except oral absorption is better Food doesnot interfere with absorption High but sustain blood levels are obtained www.indiandentalacademy.com
- 54. CLAVULONIC ACID It has rapid oral absorption and bioavailabilty of 60% ,can also be injected Plasma half 1hr and tissue distribution matches amoxcillin with which it is used ( 3rd coamoxiclav). However,it is eliminated mainly by glomerular filteration and its excretion is not effetced by pobenicid. Also. It is largely hydrolysed and decarboxylated before excretion, while amox is primarly excreted unchanged by tubular secretion www.indiandentalacademy.com
- 55. TETRACYCLINE older tetracyclines are incompletely absorbed from git Absorption is better if taken in empty stomach Dox & mino are compltely absorbed irrespective of food Tetracycline have celating propertie-insoluble and unabsorbable complexes with calcium and other metals . Milk,iron preparation, nonsystemic antacids and sucrolfate reduce their absorption www.indiandentalacademy.com
- 56. The csf conc of most tetracyclines is about one half of the plasma conc ,whether meninges are inflamed or not Most tetracyclines are excreted in urine by glomerular filteration Dose has to be reduced in renal failure;dox is an exception to this They are partly metabolized and significant amounts enter bile –some degree of enterohepatic circulation occurs They are secreted in milk I amounts sufficient to effect the suckling infant Interaction: Enzyme inducers like phenobarbitone and phenatoin enhance metabolism and reduces the half life of dox www.indiandentalacademy.com
- 57. ACYCLOVIR Only about 20% of an oral dose of acyclovir is absorbed It is plasma protein bound and is widely distributed attaining csf concentration that is 50% of plasma concentration Excreted unchanged in urine T1/2: 2-3 hrs Renal impairment necessitates dose reduction www.indiandentalacademy.com
- 58. CORTICOSTEROIDS All natural & synthetic steroids are absorbed by oral mucosa Hydrocortisone undergoes high first pass metabolism ,,90% bound to plasma Steroids are metabolised by hepatic microsomal enzymes Metabolites are excreted in urine T1/2 life is 1.5 hrs Interaction: phenobarbitone and phenytoin induce metabolism of hydrocortisone and prednisolone www.indiandentalacademy.com
- 59. MUSCLE RELAXANTS All neuromusculr blockers are not absorbed orally They are always given iv Atracurium is inactivated in plasma by spontaneous noenzymal degradation Excreted in urine n bile Interaction : thiopentone sodium & SCH should be mixed in the same syringe-react chemically www.indiandentalacademy.com