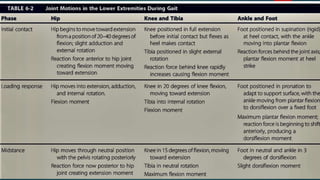
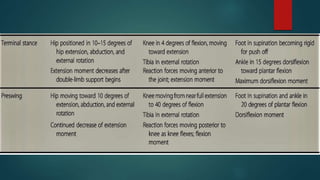
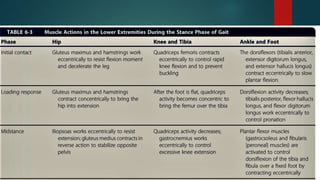
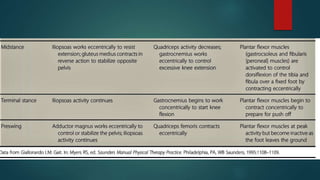
The document defines normal human gait and describes its key components and cycles. It also discusses pathological gait patterns that can result from musculoskeletal issues. Normal gait involves rhythmic movement of the limbs and trunk to propel the body forward with minimal energy expenditure. The gait cycle consists of stance and swing phases on each side. Several factors work to minimize vertical and lateral displacement of the center of gravity during walking. Pathological gaits can occur due to problems in the hips, knees, feet or ankles and result in deviations from normal gait patterns.






































































![GAIT and its different types[Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/gaitautosaved-240815185755-7939fafe-thumbnail.jpg?width=640&height=640&fit=bounds)





















