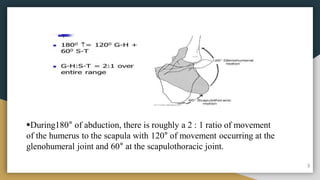
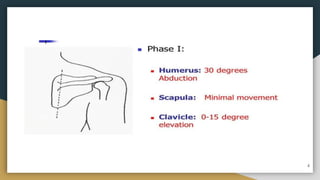
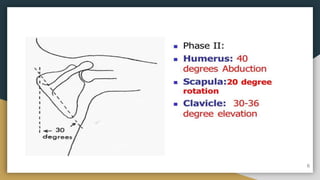
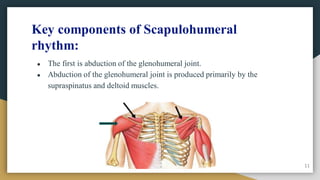
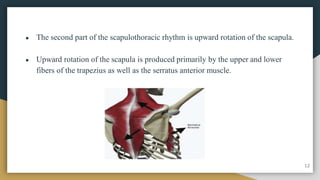
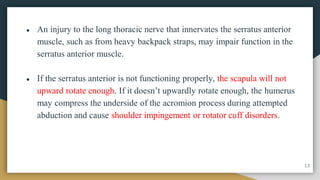
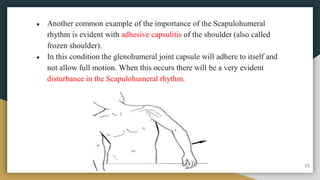
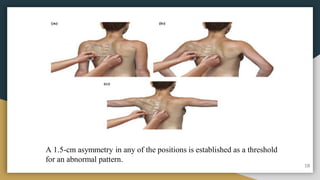
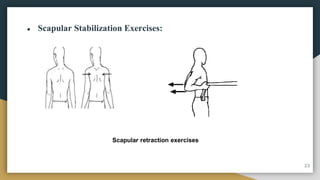
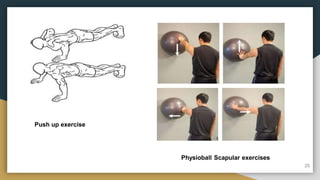
The document discusses scapulohumeral rhythm, which refers to the coordinated motion between the scapula and humerus during shoulder movement. There is typically a 2:1 ratio of humeral movement to scapular movement. Abnormal scapulohumeral rhythm can be caused by injuries or weakness and can be assessed using tests like the lateral scapular slide test and scapular dyskinesis test. Physical therapy management focuses on stretching shortened muscles and strengthening the scapular stabilizers to improve rhythm and mechanics.