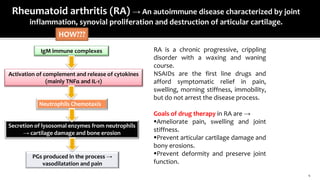
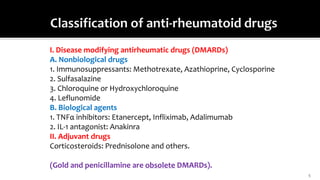
The document discusses anti-rheumatoid drugs, focusing on the classification and pharmacology of disease-modifying antirheumatic drugs (DMARDs) and adjuvant drugs, including various immunosuppressants and biological agents used in the treatment of rheumatoid arthritis (RA). It outlines the treatment goals, the mechanism of action, efficacy, potential side effects, and contraindications of each drug type, emphasizing the importance of DMARDs in managing RA symptoms and disease progression. Additionally, it highlights newer biological therapies and the role of corticosteroids in treatment strategies.