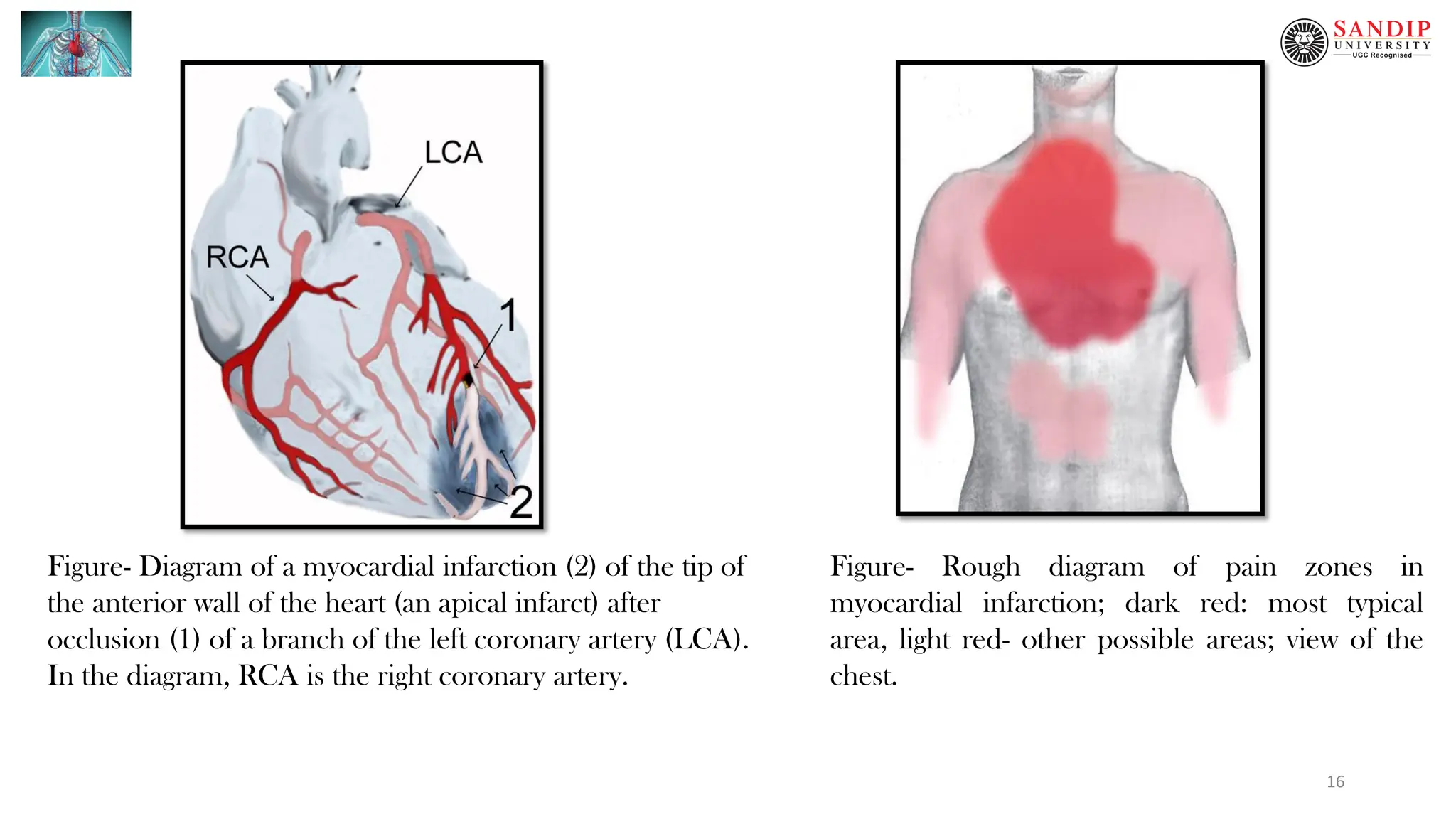
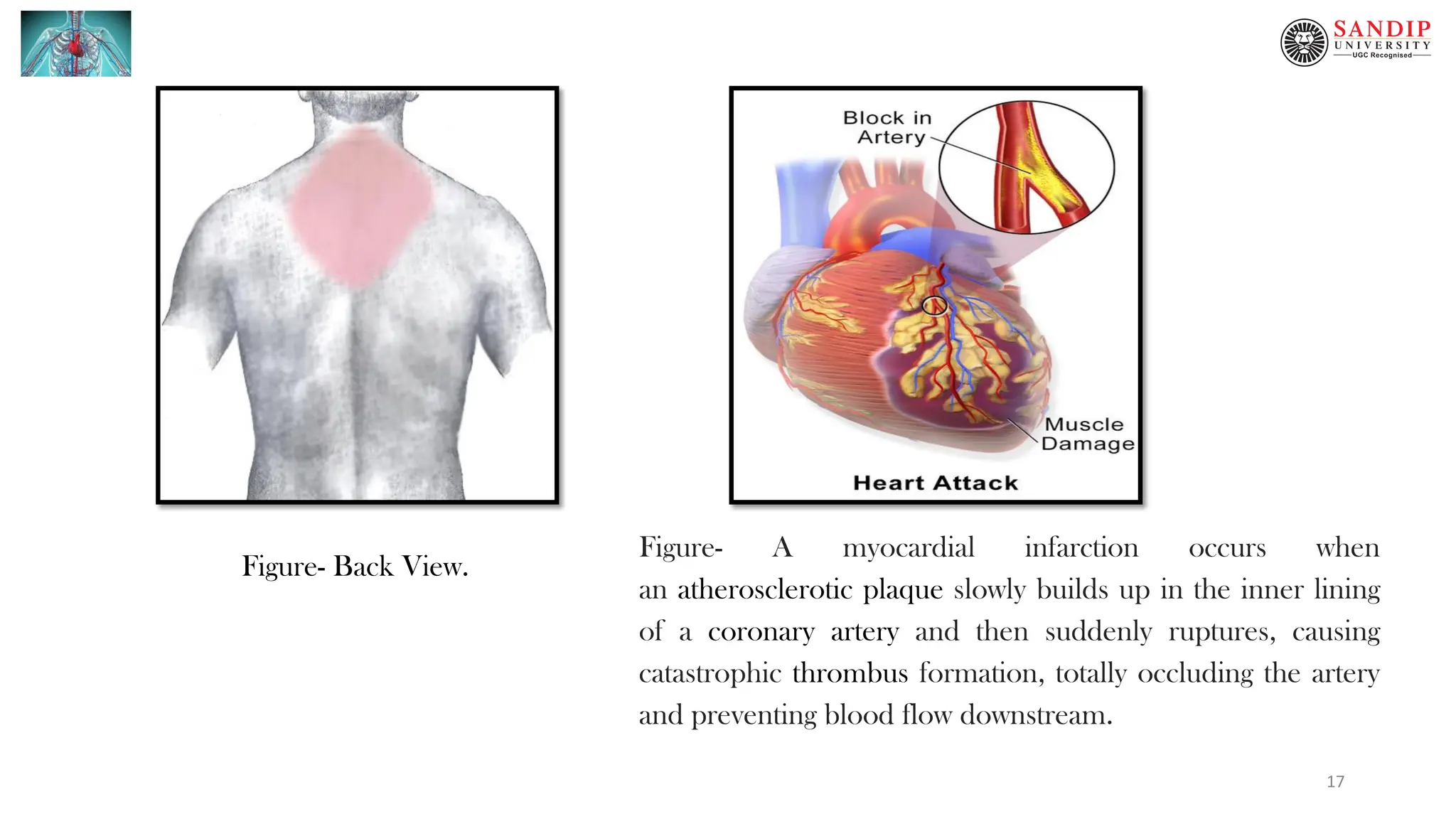
This document provides an overview of coronary artery disease (CAD) and ischemic heart disease (IHD), including their definition, clinical manifestations, and pathophysiology. CAD/IHD results from an imbalance between the heart's oxygen supply and demand. It is most commonly caused by a narrowing of the coronary arteries. The two main clinical manifestations are: 1) Angina pectoris, which presents as chest pain that occurs with exertion and is relieved by rest, and 2) Myocardial infarction (MI), commonly known as a heart attack, which is caused by cell death in the heart muscle due to lack of oxygen. MI is a medical emergency and a leading cause of death worldwide.