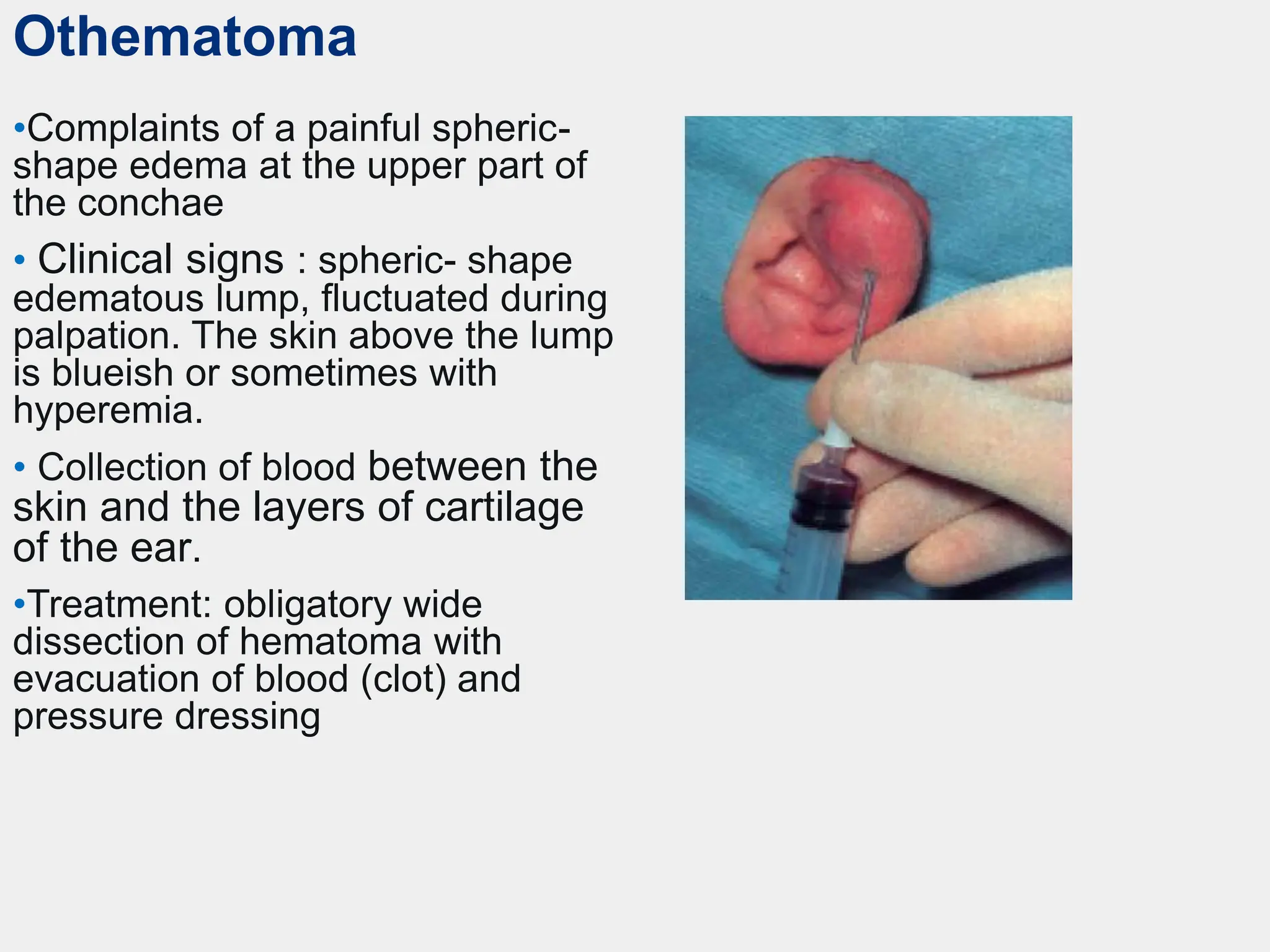
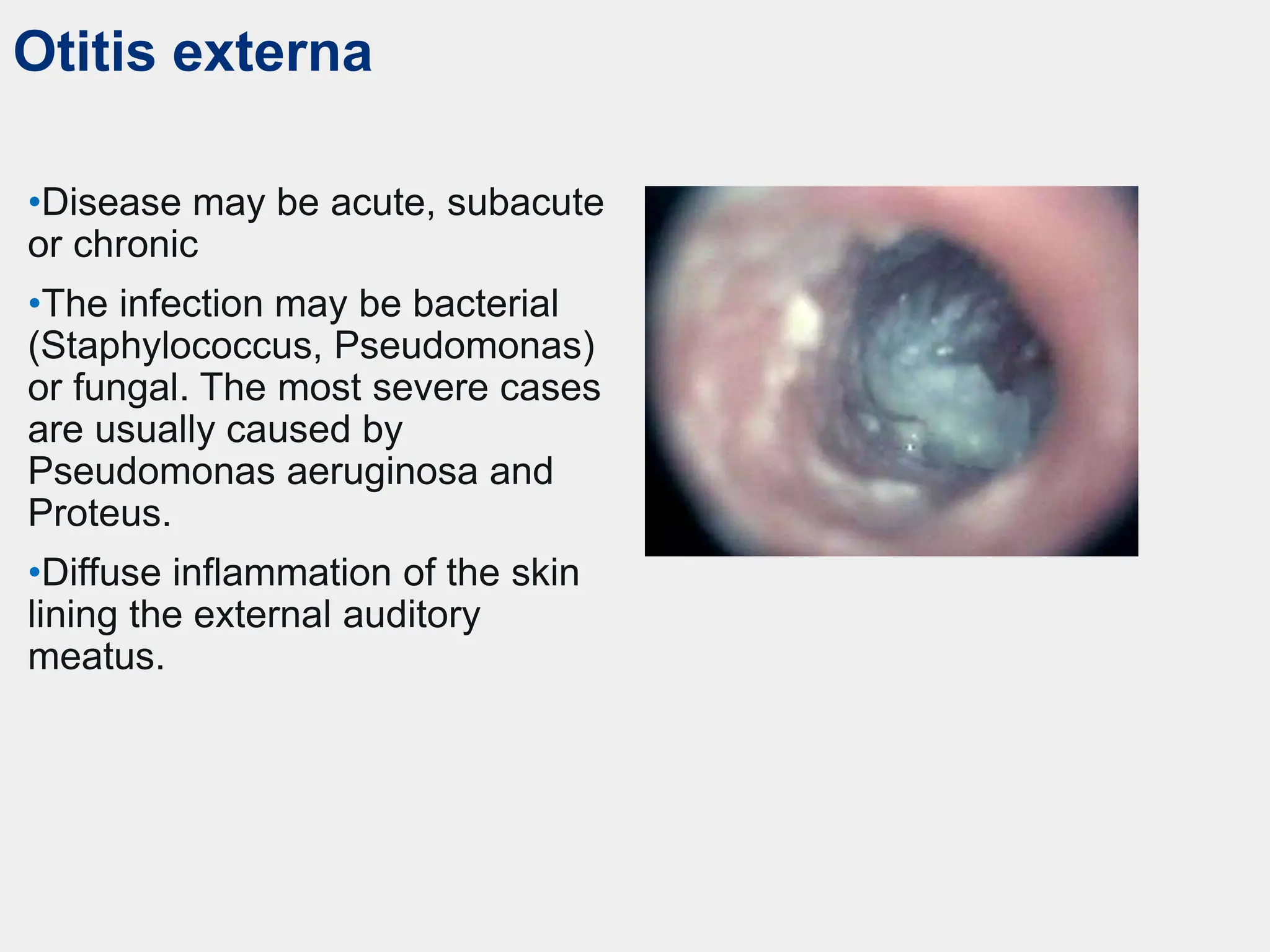
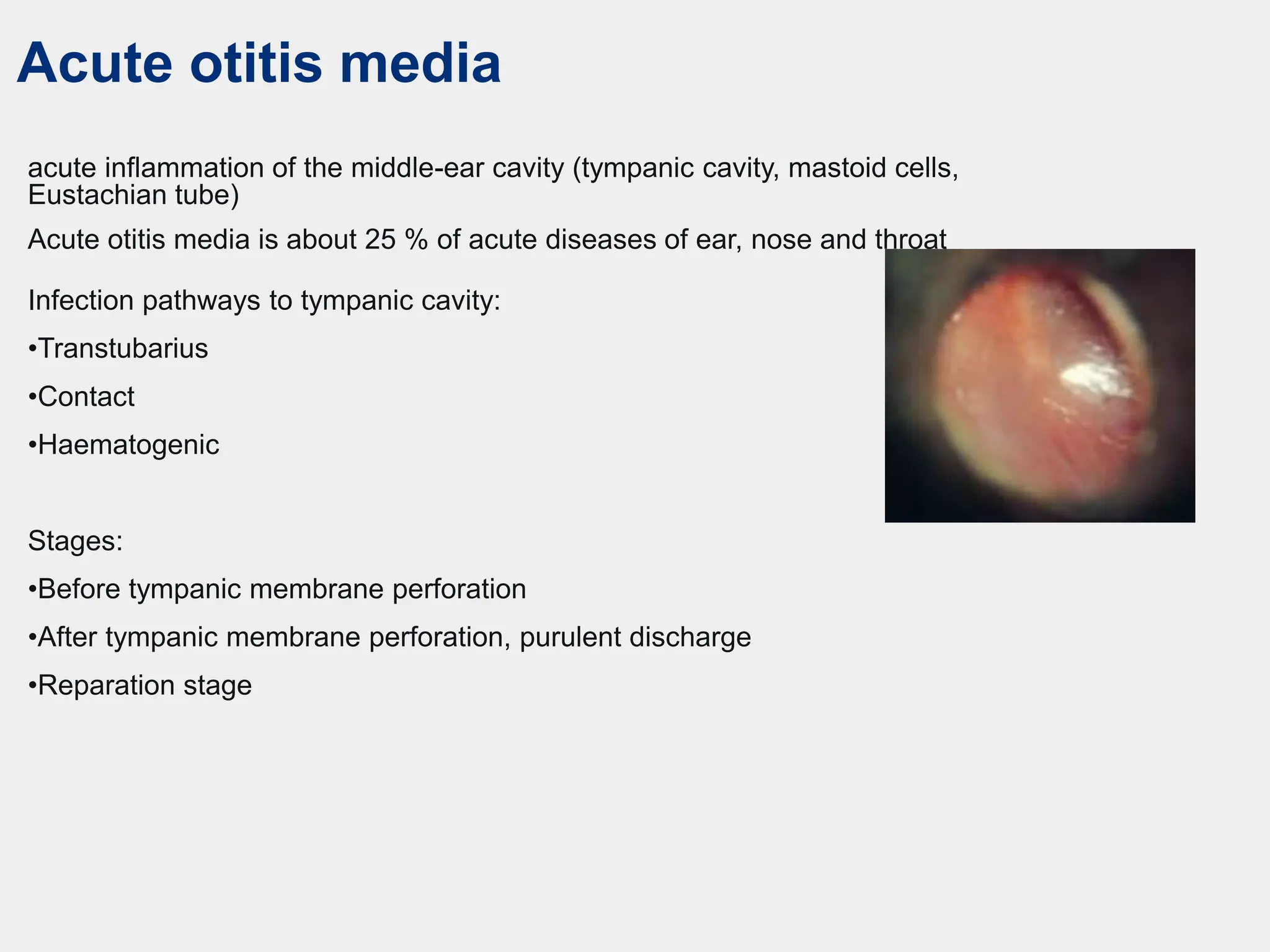
The document discusses various external ear diseases, including acute and chronic otitis media, otogenic complications, and treatments for conditions like perichondritis, eczema, and malignant otitis externa. Symptoms and stages of diseases such as acute otitis media and mastoiditis are outlined, alongside their respective treatments, including antibiotic therapy and surgical options. It emphasizes the importance of recognizing signs and managing infections effectively to prevent further complications.























































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)












