This document provides an overview of bone fractures including:
- Risk factors like age, smoking, and osteoporosis that make fractures more likely.
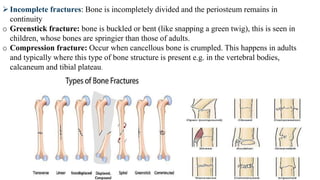
- Types of fractures like closed versus open and classifications based on location and appearance on x-rays.
- Signs and symptoms like pain, swelling, deformity, and limited mobility.
- Stages of fracture healing like inflammation, new bone formation, and remodeling over several weeks.
- Management approaches like reducing displacement, immobilizing the bones, and rehabilitation.