Faculty of ClinicalSciences
Department of Orthopedics & Trauma Medicine
Physical Traumatology I
By
James K. Mwangi
Classification of
Fractures
2.
Learning Objectives
Physical Traumatology;By the end of this unit;
Brief introduction
Define a fracture, dislocation & subluxation
Identify general causes, signs, & symptoms of fractures
Understand how fractures are identified
Explain the different fracture classifications
Understand the AO/OTA classification
Fracture Eponyms
Q & A
TAKE AWAY
3.
Introduction
What is abone?
A highly vascularized, living, constantly
changing mineralized connective tissue
It is innervated, contains vessels for
nutrition; bone cells to build up, maintain &
break down bone (important in fracture
healing).
4.
Bone tissue
Bones canbe classified based on anatomy & structure;
Anatomy
Long, short, flat, irregular bones, & sesamoid bones
Structure
Macroscopic
Cortical bone
Cancellous bone / spongy bone / trabecular bone
Microscopic
Lamellar bone
Woven bone
Bone tissue
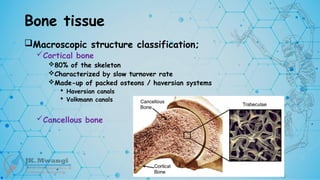
Macroscopic structureclassification;
Cortical bone
80% of the skeleton
Characterized by slow turnover rate
Made-up of packed osteons / haversian systems
Haversian canals
Volkmann canals
Cancellous bone
7.
Bone tissue
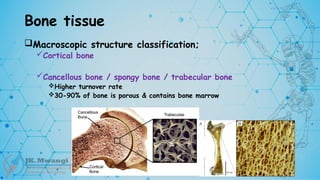
Macroscopic structureclassification;
Cortical bone
Cancellous bone / spongy bone / trabecular bone
Higher turnover rate
30-90% of bone is porous & contains bone marrow
9.
Bone tissue
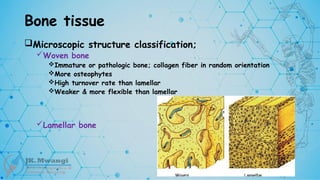
Microscopic structureclassification;
Woven bone
Immature or pathologic bone; collagen fiber in random orientation
More osteophytes
High turnover rate than lamellar
Weaker & more flexible than lamellar
Lamellar bone
10.
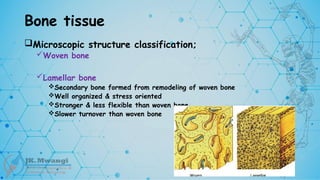
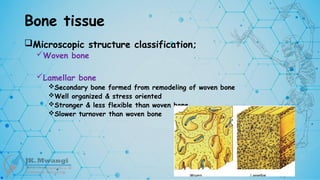
Bone tissue
Microscopic structureclassification;
Woven bone
Lamellar bone
Secondary bone formed from remodeling of woven bone
Well organized & stress oriented
Stronger & less flexible than woven bone
Slower turnover than woven bone
11.
Bone tissue
Microscopic structureclassification;
Woven bone
Lamellar bone
Secondary bone formed from remodeling of woven bone
Well organized & stress oriented
Stronger & less flexible than woven bone
Slower turnover than woven bone
12.
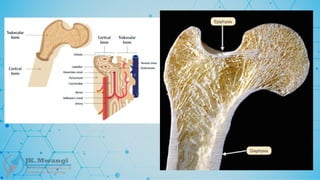
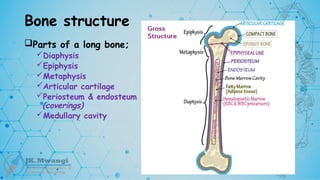
Bone structure
Parts ofa long bone;
Diaphysis
Epiphysis
Metaphysis
Articular cartilage
Periosteum & endosteum
(coverings)
Medullary cavity
Introduction
Definition
Joint dislocation
Complete lossof congruity between the articular surfaces
Joint subluxation
Loss of congruity but the 2 surfaces are still in contact
Transient subluxation
During movement, a transient subluxation may cause sudden pain & the
sensation of something ‘slipping out’, but often reduces spontaneously
Causes
Common causes offractures include;
Fall from a height
RTI
Direct injury
Repetitive force
Pathology
18.
Signs & symptoms
Whatare some of the signs & symptoms
of a fracture?
Swelling / edema
Pain & tenderness
Numbness
Bleeding
Broken skin with bone protruding
Limitation to move a limb
Other S&S are complications related
Neuropathy, compartment syndrome, red cap
refill
19.
Why classify fractures?
Toguide the treatment
To estimate the prognosis
Anticipate & mitigate possible complications
For easier communication
20.
Pathology of Fractures
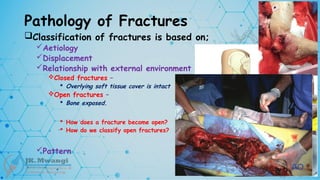
Classificationof fractures is based on;
Aetiology
Displacement
Relationship with external environment
Pattern
AO / OTA Classification
Based on eponyms
21.
Pathology of Fractures
Classificationof fractures is based on;
Aetiology
Traumatic fractures
Fragility fractures
Stress / fatigue fractures
Pathological fractures
Displacement
Relationship with external environment
Pattern
22.
Pathology of Fractures
Classificationof fractures is based on;
Aetiology
Traumatic fractures
Direct force (direct injury)
Indirect force (indirect injury)
Fragility fractures
Stress / fatigue fractures
Pathological fractures
Displacement
Relationship with external environment
Pattern
23.
Pathology of Fractures
Classificationof fractures is based on;
Aetiology
Traumatic fractures
Fragility fractures
Fractures associated with bone weakness – Osteoporosis
Stress / fatigue fractures
Pathological fractures
Displacement
Relationship with external environment
Pattern
24.
Pathology of Fractures
Classificationof fractures is based on;
Aetiology
Traumatic fractures
Fragility fractures
Stress / fatigue fractures
Normal bone – repetitive (heavy) loading, military personnel
Common sites?
• Metatarsals, shaft of tibia, shaft of fibula, & NOF
Pathological fractures
Displacement
Relationship with external environment
Pattern
26.
Pathology of Fractures
Classificationof fractures is based on;
Aetiology
Traumatic fractures
Fragility fractures
Stress / fatigue fractures
Pathological fractures
Occurs in bones weakened by a disease process – malignancy, Paget's disease,
osteogenesis imperfecta, O.M, bone cysts osteoporosis
Following trivial force / trauma or spontaneously
Displacement
Relationship with external environment
Pattern
29.
Pathology of Fractures
Classificationof fractures is based on;
Aetiology
Displacement
Undisplaced fracture – frags in contact
Displaced fracture – frags not in contact
Relationship with external environment
Pattern
30.
Pathology of Fractures
Classificationof fractures is based on;
Aetiology
Displacement
Undisplaced fracture – frags in contact
Displaced fracture – frags not in contact
Factors responsible for displacement are?
FRACTURING FORCE
MUSCLE PULL ON FRACTURE FRAGMENTS
GRAVITY
Relationship with external environment
Pattern
34.
Pathology of Fractures
Classificationof fractures is based on;
Aetiology
Displacement
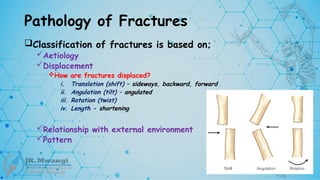
How are fractures displaced?
Relationship with external environment
Pattern
35.
Pathology of Fractures
Classificationof fractures is based on;
Aetiology
Displacement
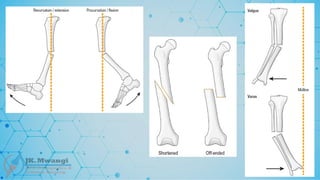
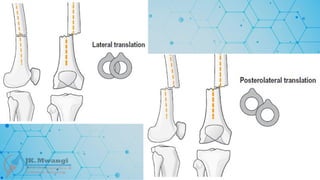
How are fractures displaced?
i. Translation (shift) – sideways, backward, forward
ii. Angulation (tilt) – angulated
iii. Rotation (twist)
iv. Length - shortening
Relationship with external environment
Pattern
48.
Pathology of Fractures
Classificationof fractures is based on;
Aetiology
Displacement
Relationship with external environment
Closed fractures –
Overlying soft tissue cover is intact
Open fractures –
Bone exposed.
How does a fracture become open?
How do we classify open fractures?
Pattern
50.
Pathology of Fractures
Classificationof fractures is based on;
Aetiology
Displacement
Relationship with external environment
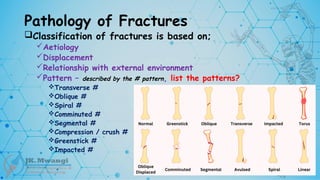
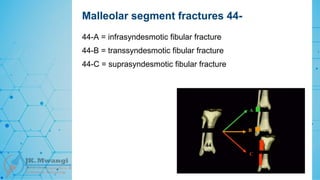
Pattern – described by the # pattern, list the patterns?
Transverse #
Oblique #
Spiral #
Comminuted #
Segmental #
Compression / crush #
Greenstick #
Impacted #
54.
AO / OTAClassification
What is OTA
Orthopaedic Trauma Association
What is AO
Association of Osteosynthesis
Reconstructive surgery aimed at stabilizing & joining the ends of a broken
bone after a fracture, an osteotomy (bone cutting procedure to realign &
reshape a bone or joint), or a non-union from a previous fracture
55.
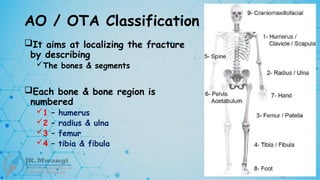
AO / OTAClassification
It aims at localizing the fracture
by describing
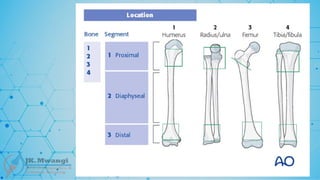
The bones & segments
Each bone & bone region is
numbered
1 – humerus
2 – radius & ulna
3 – femur
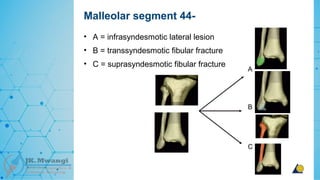
4 – tibia & fibula
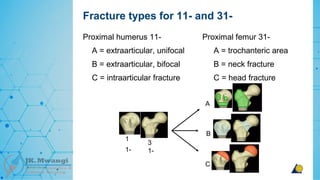
56.
AO / OTAClassification
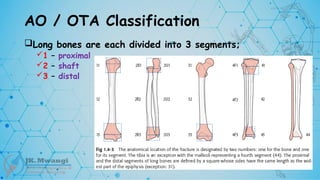
Long bones are each divided into 3 segments;
1 – proximal
2 – shaft
3 – distal
57.
AO / OTAClassification
After identifying the fractured bone and the location of
the fracture (bone & segment), next we identify the type
of fracture depending on the segment involved
Fracture type is defined as A, B, or C
58.
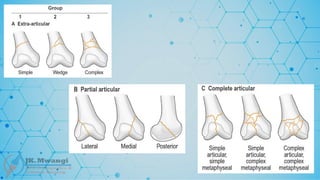
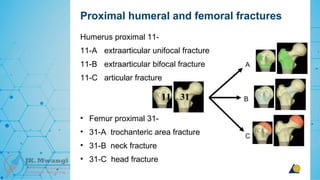
AO / OTAClassification
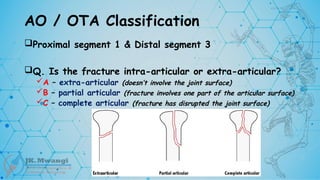
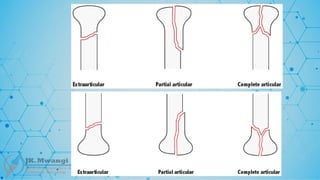
Proximal segment 1 & Distal segment 3
Q. Is the fracture intra-articular or extra-articular?
A – extra-articular (doesn’t involve the joint surface)
B – partial articular (fracture involves one part of the articular surface)
C – complete articular (fracture has disrupted the joint surface)
61.
AO / OTAClassification
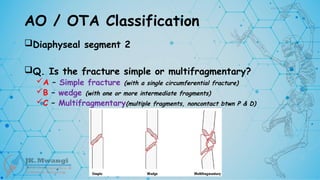
Diaphyseal segment 2
Q. Is the fracture simple or multifragmentary?
A – Simple fracture (with a single circumferential fracture)
B – wedge (with one or more intermediate fragments)
C – Multifragmentary(multiple fragments, noncontact btwn P & D)
67.
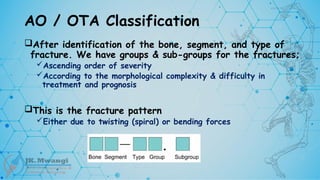
AO / OTAClassification
After identification of the bone, segment, and type of
fracture. We have groups & sub-groups for the fractures;
Ascending order of severity
According to the morphological complexity & difficulty in
treatment and prognosis
This is the fracture pattern
Either due to twisting (spiral) or bending forces
68.
AO / OTAClassification
Group;
Spiral or twisting forces will produce a
Simple spiral (X2-A1), spiral wedge (X2-B1), or spiral fragmented complex
# (X2-C1)
Bending forces produce a
Simple oblique ((X2-A2), simple transverse (X2-A3), or Bending wedge (X2-
B2), fragmented wedge (X2-B3), complex # (X2-C3)
C2 fractures in the grouping is segmental by definition
70.
AO / OTAClassification
AO summary
Which bone? H1, ru2, f3, tf4
Which segment? P1, s2, d3
Fracture type?
P & D – intra-articular, partial, complete articular = A, B, C
Shaft – simple, wedge, multifragmentary = A, B, C
Fracture group
Further defines the type
Pathology of Fractures
Fractureclassification based on eponyms
These fractures are named after individuals who either discovered
or contributed significantly to the understanding of a specific type
of fracture
What are some of the fracture eponyms?
79.
Pathology of Fractures
Fractureclassification based on eponyms
What are some of the fracture eponyms?
Colles fracture
Smiths fracture
Galeazzi fracture
Monteggia fracture
Bennett's fracture
Rolando's fracture
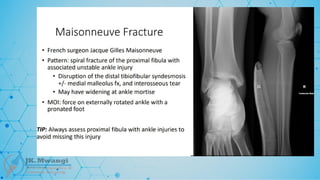
Maisonneuve fracture
Segond's fracture
Chance fracture
Boxers fracture
Chauffer's fracture (Hutchinson's fracture)
80.
Pathology of Fractures
Fractureclassification based on eponyms
What are some of the fracture eponyms?
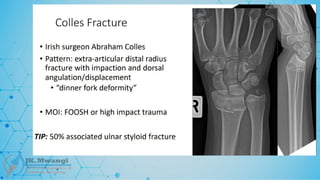
Colles fracture
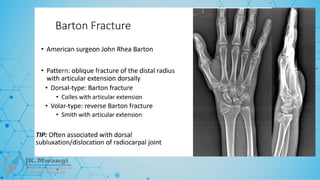
A fracture of the distal radius with dorsal (upward) displacement, often resulting
from a fall onto an outstretched hand. Named after Abraham Colles, who first
described the fracture in 1814.
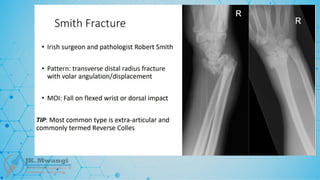
Smiths fracture
A distal radius fracture, but with volar (downward) displacement, often described
as the reverse of Colles' fracture. Named after Robert William Smith in 1847
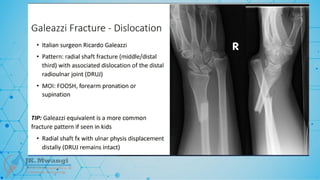
Galeazzi fracture
A fracture of the radius with associated dislocation of the distal radioulnar joint
(DRUJ). Named after Ricardo Galeazzi, who described it in 1934
81.
Pathology of Fractures
Fractureclassification based on eponyms
What are some of the fracture eponyms?
Monteggia fracture
A fracture of the proximal third of the ulna with dislocation of the radial head.
Named after Giovanni Battista Monteggia in 1814
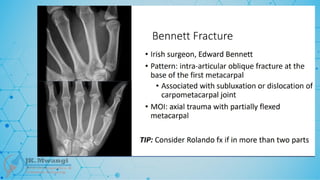
Bennetts fracture
A fracture-dislocation of the base of the first metacarpal bone (thumb), involving
the carpometacarpal (CMC) joint. Named after Edward Hallaran Bennett, who
described it in 1882
Rolando's fracture
A comminuted intra-articular fracture of the base of the first metacarpal
(thumb). It is often considered a more complex form of Bennett's fracture.
Named after Silvio Rolando.
82.
Pathology of Fractures
Fractureclassification based on eponyms
What are some of the fracture eponyms?
Potts fracture
A fracture of the lower end of the fibula, often associated with damage to the
ligaments and dislocation of the ankle. Named after Percivall Pott, an English surgeon,
in the 18th century
Maisonneuve fracture
A spiral fracture of the proximal third of the fibula associated with an ankle injury,
typically a disruption of the syndesmosis. Named after Jules Germain François
Maisonneuve, who described it in 1840.
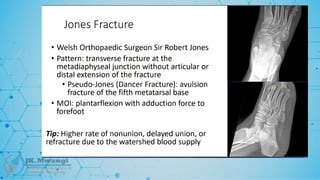
Jones fracture
A fracture at the base of the fifth metatarsal, typically caused by inversion of the
foot. Named after Sir Robert Jones, who reported it in 1902 after fracturing his own
foot.
83.
Pathology of Fractures
Fractureclassification based on eponyms
What are some of the fracture eponyms?
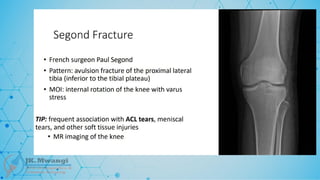
Segond's fracture
A small avulsion fracture of the lateral aspect of the tibial plateau, often
associated with anterior cruciate ligament (ACL) injuries. Named after Paul
Segond's, who first described it in 1879
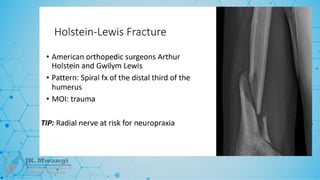
Holstein-Lewis fracture
A fracture of the distal third of the humerus, often complicated by radial nerve
injury. Named after Arthur Holstein and George Lewis, who described the
fracture in 1963.
84.
Pathology of Fractures
Fractureclassification based on eponyms
What are some of the fracture eponyms?
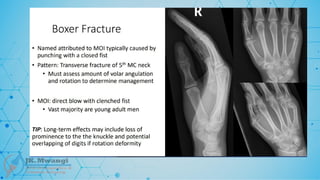
Boxers fracture
A fracture of the fifth metacarpal neck, often resulting from punching
something. Although not technically an eponym, it is colloquially referred to as
"Boxer's fracture" due to its association with fist fights.
Hutchinson's fracture (chauffeurs fracture)
An intra-articular fracture of the radial styloid. Named after Jonathan
Hutchinson. It’s also called “Chauffeur’s fracture” because it commonly occurred
in early chauffeurs when hand-cranking a car engine.
Editor's Notes
#22 traumatic fractures are the commonest in this category, and they usually occur in normal bone due to sudden and excessive force more than the ability of the bone to withstand, the trauma can be direct or indirect . When we say direct trauma this is when someone drops something heavy like a gas cylinder on the toes leading to a metatarsal fracture - so these fractures occur at the point of impact, or road traffic incident when the bumper of a vehicle hits the shin leading to a fractured tibia or tibial plateau fracture
when it comes to indirect trauma, the normal bone subjected to the external force fractures at a point distant from where the force was applied - eg a FOOSH injury leading to a fracture of the head of radius, or clavicle fracture following a fall on the shoulder.
#23 next we have fragility fractures - depending on different books you might encounter, some put together pathological fractures and fragility fractures.
but for ease of understanding in our case the fragility fractures are fractures that occur in a bone with generalized weakness due to conditions like osteoporosis, which is physiological perse and not a disease
#24 stress fractures also called fatigue fractures usually occur in normal bone which is subjected to repeated heavy loading.
these are commonly seen in athletes, military personel or dancers who have repetitive loading to the metartarsals
normally, when the bone is loaded repeatedly, very minute deformities are usually formed in the bone that initiate remodeling of the bone. ANY ONE WITH AN IDEA OF WHAT REMOELLING IS??
Remodeling is a combination of bone resorption and new bone formation in accordance to Wolffs law. WHAT IS WOLFFS LAW?
In stress fractures, the exposure to stress and deformation of bone is repeated and prolonged, this leads to bone resorption occurring faster than new bone formation
some of the commonest sites of these stress fractures are the metatarsals - where we have the famous MARCH FRACTURES, shaft of tibia and fibula, and the Neck of femur,.
as you can notice, all these are in the lower limb due to the nature of them being weight bearing
#26 and finally the Pathological fractures - these fractures usually occur through a bone that has been weakened by a disease process.
the amount of force to cause these fractures is usually very minimal and would otherwise not cause a fracture in a normal healthy bone - eg tibial fibula fracture occurring when a person stands, fracture shaft of femur when walking.
#29 When we are talking about displacement of the fracture fragments, they an either be undisplaced or displaced, this is important to know and document because it plays an important part when it comes to management of the fracture
#30 when we talk about displacement of fractures, we are basically describing what has happened to the distal fragment in relation to the proximal fragment
an undisplaced fracture is easy to identify as the bone cortex is broken but the bone is still aligned without loss of length, rotation, or angulation
but a displaced one might be easier to identify
#34 We have already mentioned some of the factors responsible for displacement to occur;
Next we will have a look at what comes next after displacement has occurred, the fragments might be displaced in a number of ways
Again, it is important to know the orientation or type of displacement because it play a big part when it comes to management of the fracture.
So how are these fracture fragments displaced? Anyone with an IDEA??
translation -
angulation -
rotation –
length
#35
So how are these fracture fragments displaced?
translation - the distal fragment is shifted sideways, backwards or forwards in relation to proximal fragment
angulation - distal fragment displaced at an angle to the proximal
rotation - distal fragment twisted along its axis. BEWARE it might look aligned on xray, but limb may end up with rotational deformity - THEREFORE ALWAYS STICK TO THE RULE OF TWOs - 2 views, 2 joints (jt above & below injury), 2 occasions, 2 sides (esp in children due to growth plates),
and lastly the length - here the fragments may be distracted and separated or may overlap due to muscle spasms causing shortening
#48 we say a fracture is closed if the overlying soft tissue cover is intact, and
open or compound when the bone is exposed, or there is a wound on the skin surface leading down to the fracture site
when we are talking about open fractures, how does a fracture become open?
it can be internally open (from within) or externally open (from outside)
internally open fractures occur when the sharp fracture fragment ends pierces the skin from within, resulting in an open fracture
and an externally open fracture occurs when the object causing the fracture lacerates the skin and soft tissue over the bone, as it breaks the bone
so, between an externally open and internally open fracture which one is more at risk and why?
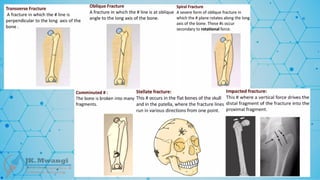
#50 transverse - the fracture line is perpendicular to the long axis of the bone
oblique - the fracture line is oblique to long axis of the bone
spiral - the fracture line runs spirally in more than 1 plane
comminuted - fracture with multiple fracture lines & resulting in multiple fragments
segmental - two fractures in one bone but at different levels
compression
greenstick - these are incomplete fractures which result in bending of the bone and not breaking
impacted - bone fragments are driven firmly together that they become interlocked & there is no movement between them