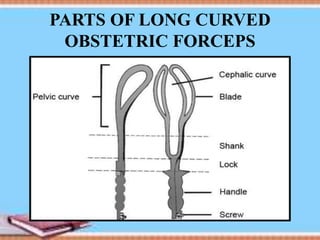
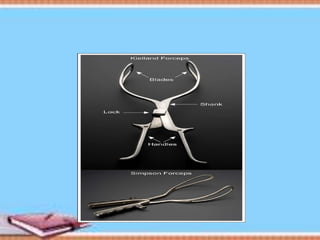
This document discusses operative vaginal delivery, specifically the use of forceps. It defines operative vaginal delivery as any delivery assisted by vaginal operations such as forceps or ventouse. It describes the different types of forceps, including long curved forceps, short curved forceps, and Kielland's forceps. It outlines the steps for performing low and outlet forceps operations. Complications for both the mother and fetus are discussed.