Manual removal of retained placenta is performed when the placenta fails to deliver within 30 minutes of childbirth. The procedure involves preparing equipment and medications, administering anesthesia and antibiotics, and manually inserting the hand into the uterus to detach and remove the placenta while supporting the uterine fundus. The provider must ensure the placenta is fully removed and the uterus remains contracted after delivery, and closely monitor the woman for complications.
The placenta is said to be retained when it is not expelled from the uterus even 30 minutes after the delivery of the baby
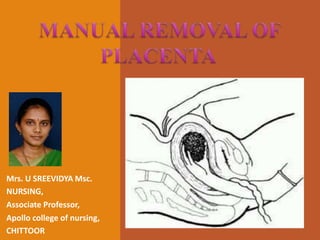
Manual placenta removal is a procedure to remove a retained placenta from the uterus after childbirth.
nurses/doctor will insert two lubricated, gloved fingers into your vagina with one hand, while the other hand presses gently on the outside of your lower abdomen. During this part of the exam, your doctor will check the size and shape of your uterus and ovaries, noting any tender areas or unusual growths.
The placenta is said to be retained when it is not expelled from the uterus even 30 minutes after the delivery of the baby
Manual placenta removal is a procedure to remove a retained placenta from the uterus after childbirth.
nurses/doctor will insert two lubricated, gloved fingers into your vagina with one hand, while the other hand presses gently on the outside of your lower abdomen. During this part of the exam, your doctor will check the size and shape of your uterus and ovaries, noting any tender areas or unusual growths.
An episiotomy is a cut (incision) through the area between your vaginal opening and your anus. This area is called the perineum. This procedure is done to make your vaginal opening larger for childbirth.
An episiotomy is a cut (incision) through the area between your vaginal opening and your anus. This area is called the perineum. This procedure is done to make your vaginal opening larger for childbirth.
The placenta is said to be retained when it is not expelled from the uterus even 30 minutes after the delivery of the baby
Manual placenta removal is a procedure to remove a retained placenta from the uterus after childbirth.
Mannual removal of placenta is done under GA.
Patient placed in lithotomy position
Bladder is catheterized
The second stage of labor begins when the cervix is completely dilated (open), and ends with the birth of your baby. Contractions push the baby down the birth canal, and you may feel intense pressure, similar to an urge to have a bowel movement. Your health care provider may ask you to push with each contraction
It is the expulsion or extraction from its mother of an embryo or fetus weighing 500 gm or less when it is not capable of independent survival (WHO).
The 500gm of fetal development is attained approximately at 22 weeks of gestation.
Expelled fetus- Abortus
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
- Video recording of this lecture in English language: https://youtu.be/lK81BzxMqdo
- Video recording of this lecture in Arabic language: https://youtu.be/Ve4P0COk9OI
- Link to download the book free: https://nephrotube.blogspot.com/p/nephrotube-nephrology-books.html
- Link to NephroTube website: www.NephroTube.com
- Link to NephroTube social media accounts: https://nephrotube.blogspot.com/p/join-nephrotube-on-social-media.html
New Drug Discovery and Development .....NEHA GUPTA
The "New Drug Discovery and Development" process involves the identification, design, testing, and manufacturing of novel pharmaceutical compounds with the aim of introducing new and improved treatments for various medical conditions. This comprehensive endeavor encompasses various stages, including target identification, preclinical studies, clinical trials, regulatory approval, and post-market surveillance. It involves multidisciplinary collaboration among scientists, researchers, clinicians, regulatory experts, and pharmaceutical companies to bring innovative therapies to market and address unmet medical needs.
These simplified slides by Dr. Sidra Arshad present an overview of the non-respiratory functions of the respiratory tract.
Learning objectives:
1. Enlist the non-respiratory functions of the respiratory tract
2. Briefly explain how these functions are carried out
3. Discuss the significance of dead space
4. Differentiate between minute ventilation and alveolar ventilation
5. Describe the cough and sneeze reflexes
Study Resources:
1. Chapter 39, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 34, Ganong’s Review of Medical Physiology, 26th edition
3. Chapter 17, Human Physiology by Lauralee Sherwood, 9th edition
4. Non-respiratory functions of the lungs https://academic.oup.com/bjaed/article/13/3/98/278874
ARTIFICIAL INTELLIGENCE IN HEALTHCARE.pdfAnujkumaranit
Artificial intelligence (AI) refers to the simulation of human intelligence processes by machines, especially computer systems. It encompasses tasks such as learning, reasoning, problem-solving, perception, and language understanding. AI technologies are revolutionizing various fields, from healthcare to finance, by enabling machines to perform tasks that typically require human intelligence.
These lecture slides, by Dr Sidra Arshad, offer a quick overview of physiological basis of a normal electrocardiogram.
Learning objectives:
1. Define an electrocardiogram (ECG) and electrocardiography
2. Describe how dipoles generated by the heart produce the waveforms of the ECG
3. Describe the components of a normal electrocardiogram of a typical bipolar leads (limb II)
4. Differentiate between intervals and segments
5. Enlist some common indications for obtaining an ECG
Study Resources:
1. Chapter 11, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 9, Human Physiology - From Cells to Systems, Lauralee Sherwood, 9th edition
3. Chapter 29, Ganong’s Review of Medical Physiology, 26th edition
4. Electrocardiogram, StatPearls - https://www.ncbi.nlm.nih.gov/books/NBK549803/
5. ECG in Medical Practice by ABM Abdullah, 4th edition
6. ECG Basics, http://www.nataliescasebook.com/tag/e-c-g-basics
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journeygreendigital
Tom Selleck, an enduring figure in Hollywood. has captivated audiences for decades with his rugged charm, iconic moustache. and memorable roles in television and film. From his breakout role as Thomas Magnum in Magnum P.I. to his current portrayal of Frank Reagan in Blue Bloods. Selleck's career has spanned over 50 years. But beyond his professional achievements. fans have often been curious about Tom Selleck Health. especially as he has aged in the public eye.
Follow us on: Pinterest
Introduction
Many have been interested in Tom Selleck health. not only because of his enduring presence on screen but also because of the challenges. and lifestyle choices he has faced and made over the years. This article delves into the various aspects of Tom Selleck health. exploring his fitness regimen, diet, mental health. and the challenges he has encountered as he ages. We'll look at how he maintains his well-being. the health issues he has faced, and his approach to ageing .
Early Life and Career
Childhood and Athletic Beginnings
Tom Selleck was born on January 29, 1945, in Detroit, Michigan, and grew up in Sherman Oaks, California. From an early age, he was involved in sports, particularly basketball. which played a significant role in his physical development. His athletic pursuits continued into college. where he attended the University of Southern California (USC) on a basketball scholarship. This early involvement in sports laid a strong foundation for his physical health and disciplined lifestyle.
Transition to Acting
Selleck's transition from an athlete to an actor came with its physical demands. His first significant role in "Magnum P.I." required him to perform various stunts and maintain a fit appearance. This role, which he played from 1980 to 1988. necessitated a rigorous fitness routine to meet the show's demands. setting the stage for his long-term commitment to health and wellness.
Fitness Regimen
Workout Routine
Tom Selleck health and fitness regimen has evolved. adapting to his changing roles and age. During his "Magnum, P.I." days. Selleck's workouts were intense and focused on building and maintaining muscle mass. His routine included weightlifting, cardiovascular exercises. and specific training for the stunts he performed on the show.
Selleck adjusted his fitness routine as he aged to suit his body's needs. Today, his workouts focus on maintaining flexibility, strength, and cardiovascular health. He incorporates low-impact exercises such as swimming, walking, and light weightlifting. This balanced approach helps him stay fit without putting undue strain on his joints and muscles.
Importance of Flexibility and Mobility
In recent years, Selleck has emphasized the importance of flexibility and mobility in his fitness regimen. Understanding the natural decline in muscle mass and joint flexibility with age. he includes stretching and yoga in his routine. These practices help prevent injuries, improve posture, and maintain mobilit
Flu Vaccine Alert in Bangalore Karnatakaaddon Scans
As flu season approaches, health officials in Bangalore, Karnataka, are urging residents to get their flu vaccinations. The seasonal flu, while common, can lead to severe health complications, particularly for vulnerable populations such as young children, the elderly, and those with underlying health conditions.
Dr. Vidisha Kumari, a leading epidemiologist in Bangalore, emphasizes the importance of getting vaccinated. "The flu vaccine is our best defense against the influenza virus. It not only protects individuals but also helps prevent the spread of the virus in our communities," he says.
This year, the flu season is expected to coincide with a potential increase in other respiratory illnesses. The Karnataka Health Department has launched an awareness campaign highlighting the significance of flu vaccinations. They have set up multiple vaccination centers across Bangalore, making it convenient for residents to receive their shots.
To encourage widespread vaccination, the government is also collaborating with local schools, workplaces, and community centers to facilitate vaccination drives. Special attention is being given to ensuring that the vaccine is accessible to all, including marginalized communities who may have limited access to healthcare.
Residents are reminded that the flu vaccine is safe and effective. Common side effects are mild and may include soreness at the injection site, mild fever, or muscle aches. These side effects are generally short-lived and far less severe than the flu itself.
Healthcare providers are also stressing the importance of continuing COVID-19 precautions. Wearing masks, practicing good hand hygiene, and maintaining social distancing are still crucial, especially in crowded places.
Protect yourself and your loved ones by getting vaccinated. Together, we can help keep Bangalore healthy and safe this flu season. For more information on vaccination centers and schedules, residents can visit the Karnataka Health Department’s official website or follow their social media pages.
Stay informed, stay safe, and get your flu shot today!
NVBDCP.pptx Nation vector borne disease control programSapna Thakur
NVBDCP was launched in 2003-2004 . Vector-Borne Disease: Disease that results from an infection transmitted to humans and other animals by blood-feeding arthropods, such as mosquitoes, ticks, and fleas. Examples of vector-borne diseases include Dengue fever, West Nile Virus, Lyme disease, and malaria.
3. Manual placenta removal is a
procedure to remove a retained
placenta from the uterus after childbirth
4.
• Take blood for grouping and cross match and send
for hemoglobin if it has not been done
Tell the woman (and her support person) what is
going to be done, listen to her and respond
attentively to her questions and concerns.
• Provide continual emotional support and
reassurance, as feasible.
5. Prepare the necessary equipment
• Antiseptic solution
• Sterile gloves
• Blood and subtitutes
• Anasthesia and analgesics
• Ergometrine and oxytocin
Antibiotics
6.
Give anesthesia (IV pethidine (25-50mg) and
diazepam (10 mg), or ketamine
Give a single dose of prophylactic antibiotics: Ampicillin
2 g IV PLUS metronidazole 500 mg IV, OR
Cefazolin 1 g IV PLUS metronidazole 500 mg IV
Put on personal protective equipment.
7. Procedure is done under GA
If not available under deep sedation
Patient placed in lithotomy position
Bladder is catheterized
8. Use antiseptic hand rub or wash hands and forearms.
Put high-level disinfected or sterile surgical gloves on
both hands. (Note: elbow-length gloves should be
used, if available.)
Hold the umbilical cord with a clamp
Pull the cord gently until it is parallel to the floor
9. Place the fingers of one hand into the vagina
in the shape of cone by drawing the fingers and the
thumb together and into the uterine cavity, following
the direction of the cord until the placenta is located.
11. When the placenta has been located, let go
of the cord and move that hand onto the abdomen to
support the fundus abdominally and to provide counter-
traction to prevent uterine inversion .
Move the fingers of the hand in the uterus laterally
until the edge of the placenta is located. Supporting the
fundus while detaching the placenta
13. Keeping the fingers tightly together, ease the edge
of the hand gently between the placenta and the uterine
wall, with the palm facing the placenta.
Gradually move the hand back and forth in a
smooth lateral motion until the whole placenta is separated
from the uterine wall withdrawing the hand from the uterus
14.
15. When the placenta is completely separated
Palpate the inside of the uterine cavity to ensure that all
placental tissue has been removed.
Slowly withdraw the hand from the uterus bringing the
placenta with it.
Continue to provide counter-traction to the fundus by
pushing it in the opposite direction of the hand that is
being withdrawn.
16. Give oxytocin 20 units in 1 L IV fluid (normal saline or
Ringer’s lactate) at 60 drops/minute.
Massage the fundus to encourage atonic uterine
contraction.
If there is continued heavy bleeding- Give ergometrine
0.2 mg IM or give prostaglandins.
Examine the uterine surface of the placenta to ensure that
it is complete. Examine the woman carefully and repair
any tears to the cervix or vagina, or repair episiotomy.
17. Examine the placenta for
completeness
Check for contracted uterus
18. Immerse both gloved hands in 0.5%
chlorine solution. Remove gloves by
turning them inside out.
If disposing of gloves, place them in a
leak proof container or plastic bag.
If reusing surgical gloves, submerge
them in 0.5% chlorine solution for 10
minutes for decontamination
19. Use antiseptic hand rub or wash hands thoroughly
with soap and water and dry with a clean, dry
cloth or air dry.
Monitor vaginal bleeding and take the woman’s
vital signs:
Every 15 minutes for 1 hour
Then every 30 minutes for 2 hours
Make sure that the uterus is firmly contracted.
Record procedure and findings on woman’s record.
20. Observe the woman closely until the effect of IV
sedation has worn off.
Monitor the vital signs (pulse, blood pressure,
respiration) every 30 minutes for the next 6 hours or
until stable.
Palpate the uterine fundus to ensure that the uterus
remains contracted.
Check for excessive lochia.
Continue infusion of IV fluids.
Transfuse as necessary.