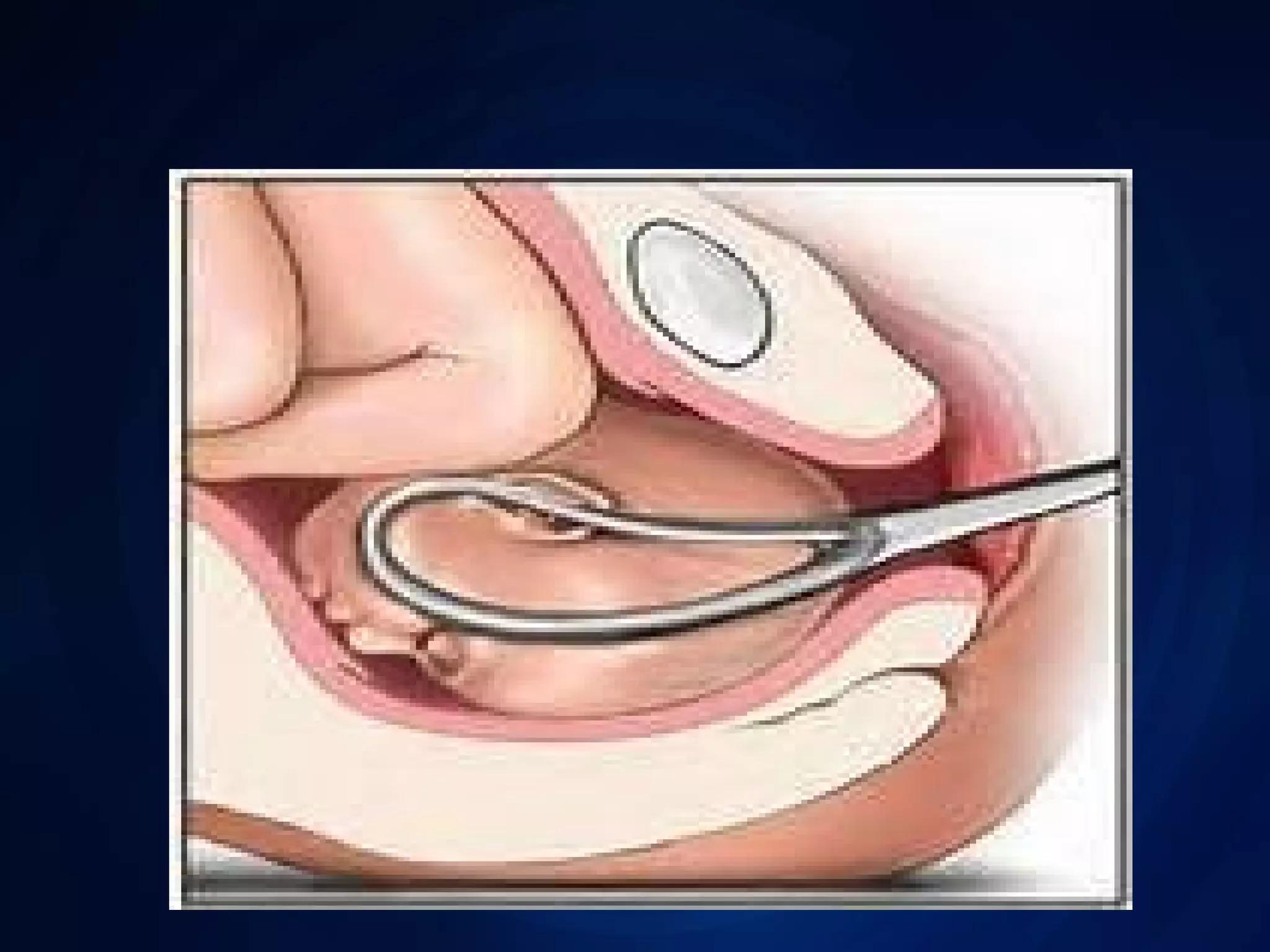
This document discusses forceps delivery, which is an assisted birth using obstetric forceps to extract the fetal head when the mother is unable to deliver the baby on her own. It describes the different types of forceps used based on how far the baby's head has descended in the birth canal, including high, mid, low, rotational, and outlet forceps. The indications for a forceps delivery include maternal conditions like exhaustion or fetal distress. Criteria that must be met first include a fully dilated cervix. Complications can be maternal like vaginal lacerations or postpartum hemorrhage, or fetal like bruising, hemorrhage, or asphyxia.