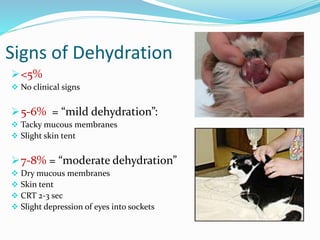
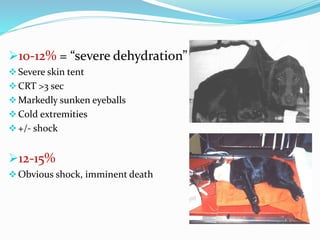
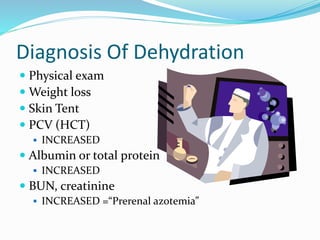

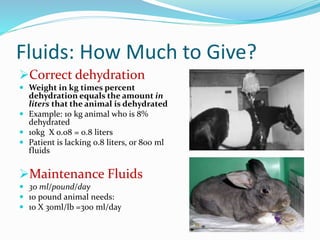
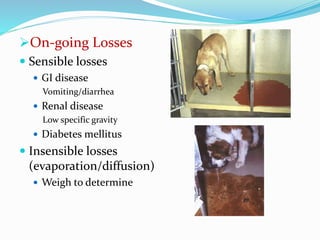


This document discusses fluid therapy in veterinary medicine. It begins by explaining that fluids are given during surgery to prevent hypotension and acid-base abnormalities. Fluids are also given at other times to correct dehydration, electrolyte imbalances, or deliver drugs. The document then describes signs of dehydration from mild to severe and how to diagnose dehydration. It provides guidance on calculating fluid needs and types of fluids including crystalloids, colloids, lactated Ringer's solution, and 0.9% saline. The document concludes by covering administration routes, calculating flow rates, and daily monitoring of patients receiving fluids.























































































