
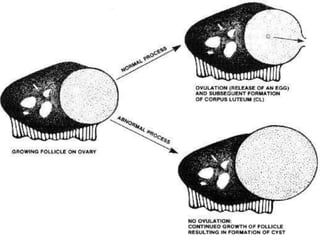
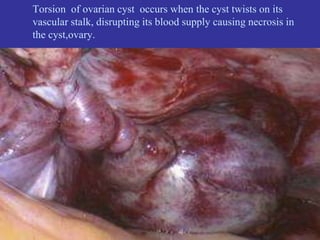
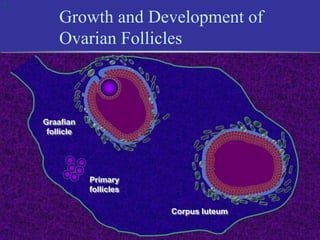
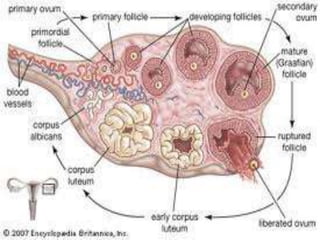
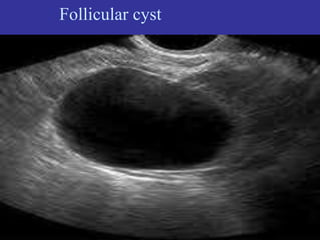
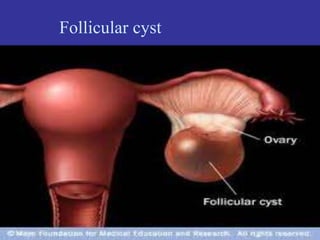
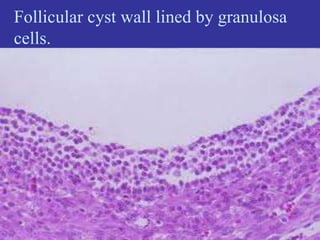
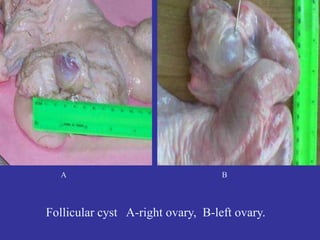
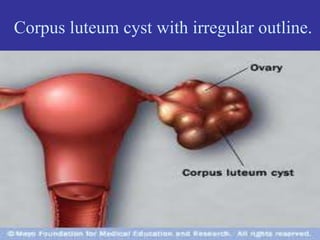
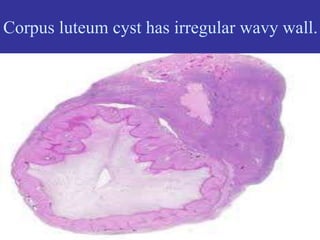

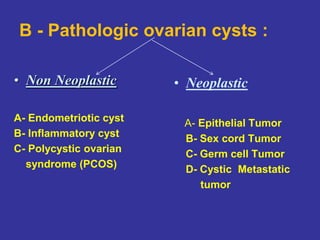



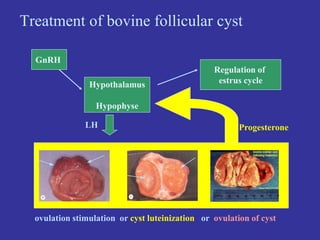

This document discusses ovarian cysts in cattle. It begins by defining ovarian cysts as fluid-filled sacs arising from the ovary that are usually over 25mm in diameter. The two main types of physiologic ovarian cysts are follicular cysts, which form when a follicle does not rupture to release an egg, and corpus luteum cysts, which form if the corpus luteum does not dissolve after ovulation. Pathologic cysts can cause pain, infertility, or torsion of the cyst. The document then discusses various types of pathologic cysts and differences between benign and malignant ovarian cysts in cattle. Treatment options for follicular cysts in cattle include GnRH or PGF2α to induce ovulation or























































































