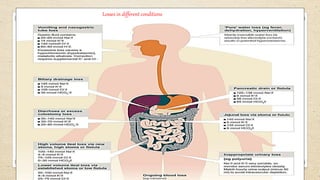
1) The document discusses fluid management, summarizing water intake and output in the human body and types of intravenous fluids used.
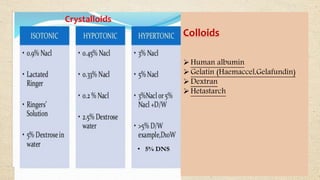
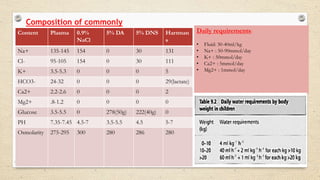
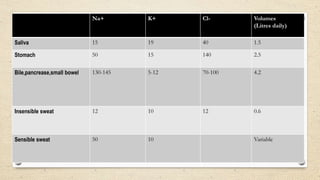
2) It provides details on crystalloid and colloid solutions, as well as the composition of commonly used crystalloids.
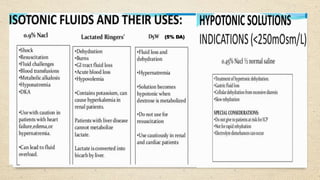
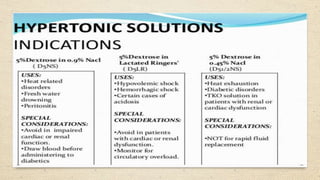
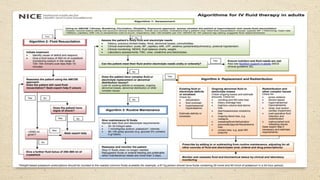
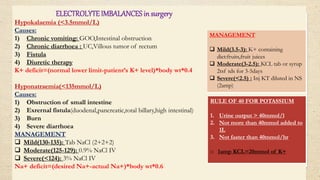
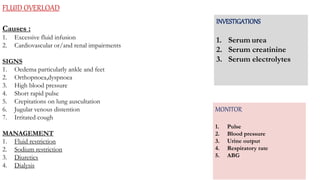
3) Preferred intravenous fluids for different conditions are outlined, along with fluid regimen calculations and management of electrolyte imbalances that can occur during surgery.