What is fluid?
Anyliquid, gas, or material that
cannot sustain a tangential, or
shearing, force at rest and
undergoes a continuous change in
shape when subjected to such
stress.
What is Fluid Therapy?
Fluid therapy is the administration
of fluids to a patient as a treatment
or preventative measure.
It can be administered via
intravenous, intraperitoneal,
intraosseous, subcutaneous, and
oral routes.
What is Fluid Therapy?
3.
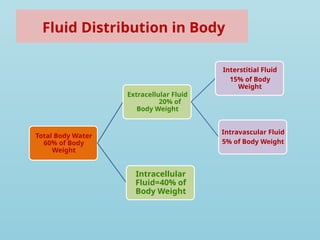
Fluid Distribution inBody
Total Body Water
60% of Body
Weight
Extracellular Fluid
20% of
Body Weight
Interstitial Fluid
15% of Body
Weight
Intravascular Fluid
5% of Body Weight
Intracellular
Fluid=40% of
Body Weight
4.
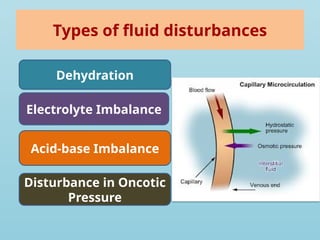
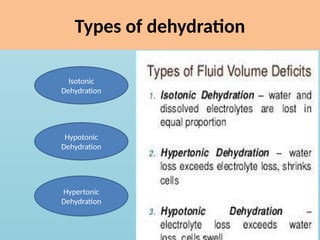
Types of fluiddisturbances
Dehydration
Electrolyte Imbalance
Acid-base Imbalance
Disturbance in Oncotic
Pressure
5.
Intravenous fluids
Intravenousfluids are chemically prepared
solutions that are administered to the patient.
They are tailored to the body’s needs and
used to replace lost fluids and/or aid in the
delivery of IV medications.
6.
INDICATIONS OF FLUIDTHERAPY
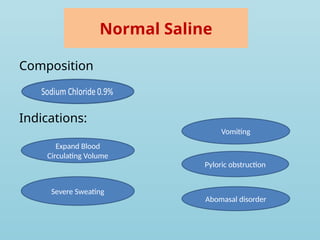
For rapid restoration of fluid and electrolytes
in dehydration due to vomiting, diarrhea,
shock due to hemorrhage or sepsis or burns.
Total parenteral nutrition.
Anaphylaxis, cardiac arrest, hypoxia.
Post gastrointestinal surgeries.
For maintenance, replacement of loss or as a
special fluid.
7.
Advantages of fluidtherapy
Provides the patient with life-sustaining fluids,
electrolytes, and drugs.
Immediate and predictable therapeutic effects.
Preferred for administering fluids, electrolytes,
and drugs in emergencies.
Allow fluid intake when the patient has GI
malabsorption.
IV Fluids
Themajority of an IV solution is sterile water.
Solvent and solute
Solvent is water
Solutes can be molecules called electrolytes
or other large compounds such as proteins or
molecules.
10.
Intravenous Fluids
IVfluids come in three different forms
Colloids
Crystalloids
Blood and blood products
11.
Colloidal Solutions
Colloidsolutions are IV fluids containing large
proteins and molecules that tend to stay
within the vascular space (blood vessels).
They shift the fluids from the interstitial to the
intravascular compartment
Colloids are useful in maintaining blood
volume.
Colloids are expensive, have specific storage
requirements, and have a short shelf life.
Commonly used colloids include plasma
proteins, salt-poor albumin, and dextran.
12.
Crystalloid Solution
Crystalloidsolutions are primarily fluids used
for IV therapy.
Contains electrolytes but lacks the large
proteins and molecules found in colloids.
Crystalloids come in different preparations
and are classified according to their “tonicity”.
A crystalloid’s tonicity describes the
concentration of electrolytes dissolved in
water, as compared with that of body plasma.
13.
Blood and BloodProducts
When PCV decreases then there is a need of
blood transfusion. In severe anemia: where
there is extreme depletion of oxygen carrying
capacity of the blood occurs & life is
threatened.
PCV between 10 & 15% will benefit from a
transfusion.
Normal PCV of Ruminants is 24-46% and of
equines 32-48%.
14.
Isotonic Solutions
Tonicityequal to plasma
Even distribution between intravascular space
and plasma.
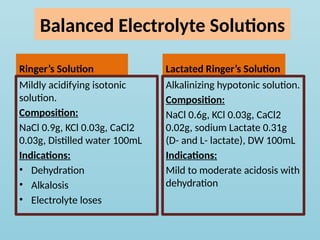
5% dextrose
Lactated ringer
Normal saline
15.
Hypotonic Solutions
Tonicitylower than body plasma
Shift from intravascular space to
extravascular space and then to cell.
0.45% NaCl
Used for dehydration
16.
Hypertonic Solutions
Tonicityhigher than body plasma
Cause the water to shift from extravascular
space into the bloodstream, increasing
intravascular volume.
5% dextrose in 0.45% NaCl
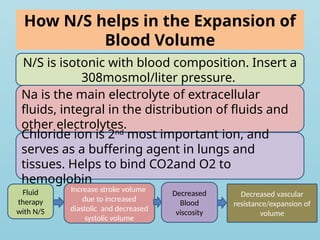
How N/S helpsin the Expansion of
Blood Volume
Fluid
therapy
with N/S
Increase stroke volume
due to increased
diastolic and decreased
systolic volume
Decreased
Blood
viscosity
Decreased vascular
resistance/expansion of
volume
N/S is isotonic with blood composition. Insert a
308mosmol/liter pressure.
Na is the main electrolyte of extracellular
fluids, integral in the distribution of fluids and
other electrolytes.
Chloride ion is 2nd
most important ion, and
serves as a buffering agent in lungs and
tissues. Helps to bind CO2and O2 to
hemoglobin
22.
• NaCl ismild acidifying as effective.
• Has little merit in routine treatment of
ruminants, as ruminants develop
hypokalemia and hypocalcemia when
inappetent.
• Can act as a vehicle for adding other
electrolytes and dextrose.
23.
Contraindications to theUse of N/S
Impaired Kidney Functions
Congestive heart failure, can lead to
pulmonary edema
If infused in too large quantities can lead to
net acidosis
• Dextrose injectedparenterally oxidized to
carbon dioxide and water. Sodium chloride
provides sodium and chlorine.
• Used in mild diarrhea as in this case loss of
sodium ions occurs. Na is the principal cation
of extracellular fluid
Mechanism of Actionof Ringer
Solution
SID ( Effective strong ion difference): it is the strong
difference between the cation and strong anion
concentration after metabolized anions have been
completely metabolized to produce bicarbonate. Solutions
having SID greater than 27mEq/L are alkalinizing. Solutions
having SID=0 are acidifying.
Ringer solution SID= 0mEq/L. so acidifying in nature.
Adult ruminants tend to get alkalemic when inappetent so
this solution will be preferred.
As containing major electrolytes required by the body so
helps in electrolyte balance.
Helps in rehydration as containing sodium helps in the
expansion of blood volume.
28.
Mechanism of actionof Lactated Ringer
Solution
Osmolality 275 mOsmol/L.
It is alkalinizing as lactate metabolizes into
bicarbonate ion.
Standard intravenous solution for neonates
and horses, as these become acidemic when
inappetent.
29.
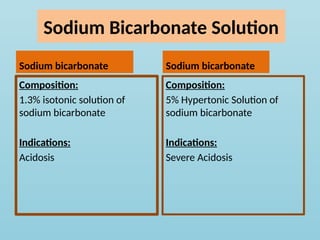
Sodium Bicarbonate Solution
Sodiumbicarbonate
Composition:
1.3% isotonic solution of
sodium bicarbonate
Indications:
Acidosis
Sodium bicarbonate
Composition:
5% Hypertonic Solution of
sodium bicarbonate
Indications:
Severe Acidosis
30.
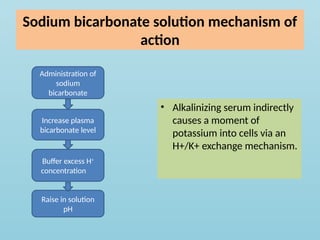
Sodium bicarbonate solutionmechanism of
action
• Alkalinizing serum indirectly
causes a moment of
potassium into cells via an
H+/K+ exchange mechanism.
Administration of
sodium
bicarbonate
Increase plasma
bicarbonate level
Buffer excess H+
concentration
Raise in solution
pH
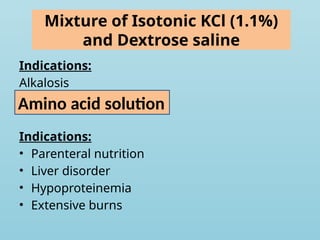
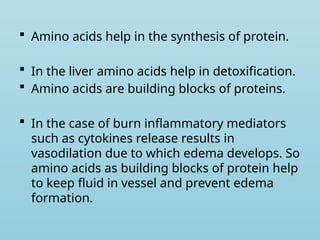
Amino acidshelp in the synthesis of protein.
In the liver amino acids help in detoxification.
Amino acids are building blocks of proteins.
In the case of burn inflammatory mediators
such as cytokines release results in
vasodilation due to which edema develops. So
amino acids as building blocks of protein help
to keep fluid in vessel and prevent edema
formation.
Dextran
High molecularweight glucose
polymers formed by fermentation
of sucrose.
As mol. Wt. is similar to albumin
therefore limiting diffusion into
interstitial spaces. Results in
increased oncotic pressure in
blood vessels, due to which fluid
stays in vessels.
Act as a plasma volume expander
in contrast to crystalloids, which
expand extracellular fluid volume.
Haemacel
• Shorter plasma half
life than dextran
Mechanism of actionof mannitol
• It elevates blood plasma osmolality, resulting
in enhanced flow of water from tissues,
including the brain and cerebrospinal fluids,
into interstitial fluids and plasma.
39.
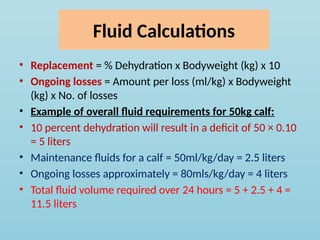
Fluid Calculations
• Replacement= % Dehydration x Bodyweight (kg) x 10
• Ongoing losses = Amount per loss (ml/kg) x Bodyweight
(kg) x No. of losses
• Example of overall fluid requirements for 50kg calf:
• 10 percent dehydration will result in a deficit of 50 × 0.10
= 5 liters
• Maintenance fluids for a calf = 50ml/kg/day = 2.5 liters
• Ongoing losses approximately = 80mls/kg/day = 4 liters
• Total fluid volume required over 24 hours = 5 + 2.5 + 4 =
11.5 liters
40.
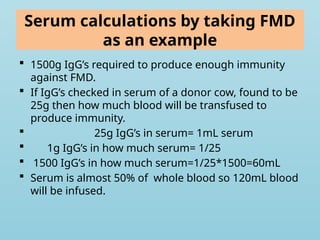
Serum calculations bytaking FMD
as an example
1500g IgG’s required to produce enough immunity
against FMD.
If IgG’s checked in serum of a donor cow, found to be
25g then how much blood will be transfused to
produce immunity.
25g IgG’s in serum= 1mL serum
1g IgG’s in how much serum= 1/25
1500 IgG’s in how much serum=1/25*1500=60mL
Serum is almost 50% of whole blood so 120mL blood
will be infused.
41.
Blood transfusion calculations
Total Volume Infused= ([Patient PCV-Minimum
PCV]/Patient PCV)*Blood Volume
Blood Volume is 7-9% of body weight.



![Blood transfusion calculations
Total Volume Infused= ([Patient PCV-Minimum
PCV]/Patient PCV)*Blood Volume
Blood Volume is 7-9% of body weight.](https://image.slidesharecdn.com/clinicfluidtherapy-11-250523041545-b56031c1/85/Clinic-Fluid-Therapy-its-clincal-application-41-320.jpg)





















































