



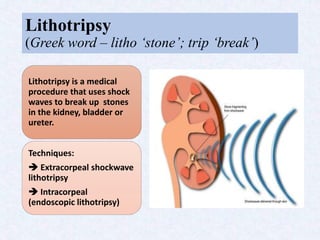
































Laser lithotripsy uses a laser to fragment urinary stones into smaller pieces that can pass through the urinary tract. There are two main types - extracorporeal shockwave lithotripsy which uses external shockwaves, and intracorporeal (endoscopic) lithotripsy where a laser fiber is inserted. Laser lithotripsy is preferred over open surgery as it is less invasive and allows visualization. Settings like pulse energy, frequency, and width can be adjusted for different stone compositions and locations. While effective, risks include injury to surrounding tissue and accidental fiber breakage.























































































