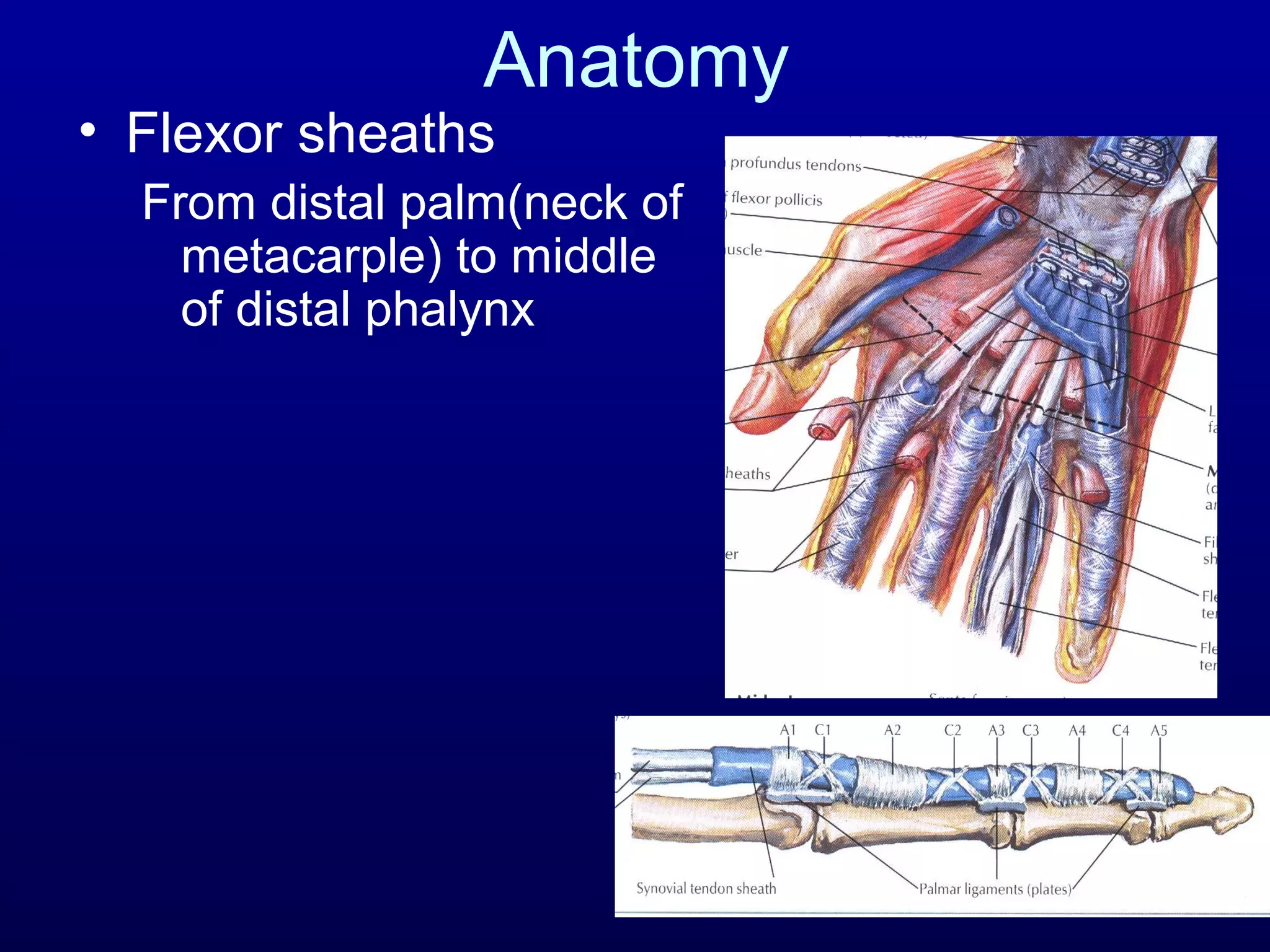
This document discusses flexor tendon injuries. It covers anatomy of the flexor tendons and pulley system. It describes zones of injury, techniques for repair, and post-operative rehabilitation. For zone 2 injuries or when primary repair is not possible, options include tenolysis to release adhesions, tendon transfers, or single-stage tendon grafting using a smaller caliber graft passed through the pulley system. The goals are to perform a strong repair, minimize adhesions, and allow early controlled motion to promote healing.