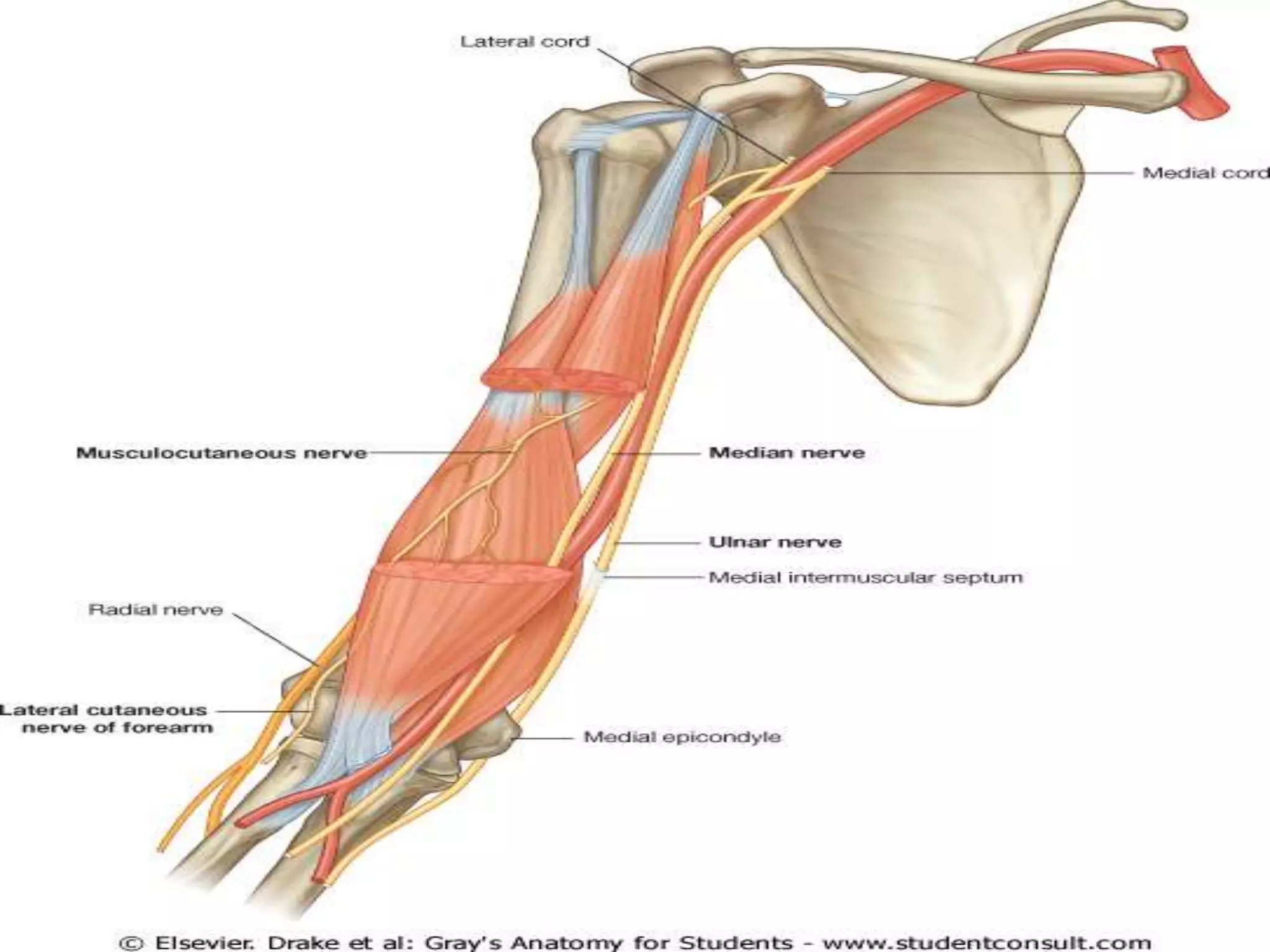
This document provides an overview of median nerve injuries, including anatomy, types of injuries, clinical examination findings, and management principles. It describes the anatomy of the median nerve from its origins in the brachial plexus through the arm, forearm, and hand. It discusses high and low median nerve injuries. Key examination techniques are outlined, including tests for specific muscle function. Surgical management principles include nerve repair, decompression, and tendon transfers. Common compression neuropathies like carpal tunnel syndrome and pronator teres syndrome are also summarized, including their symptoms, diagnosis, and treatment.






























































































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)
