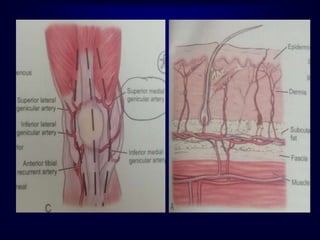
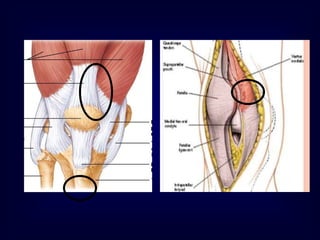
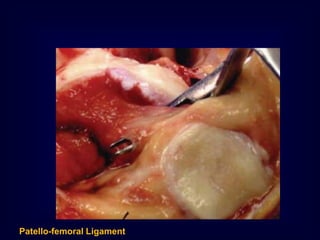
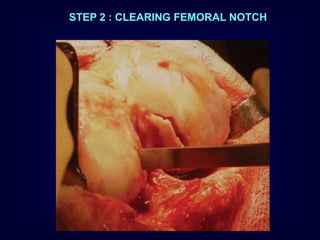
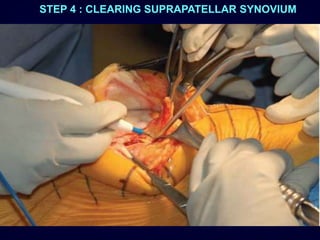
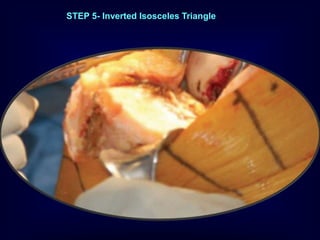
1. The document describes the basic surgical technique for total knee arthroplasty (TKA), including the medial parapatellar approach and steps for femoral and tibial bone cuts.
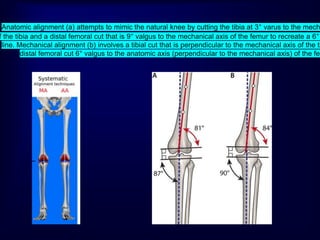
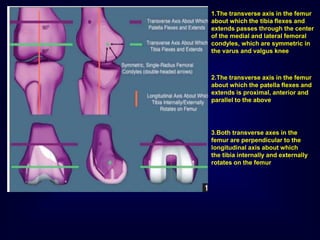
2. It discusses different alignment techniques in TKA including anatomical, mechanical, and kinematic alignment. Kinematic alignment aims to restore the natural three motion axes of the knee.
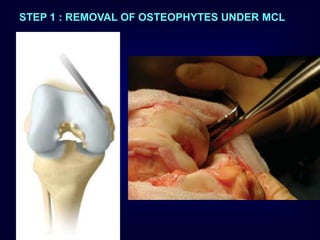
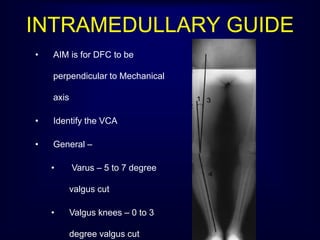
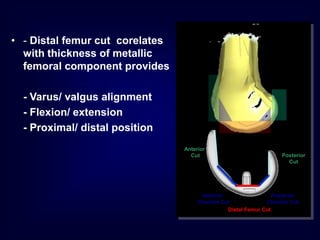
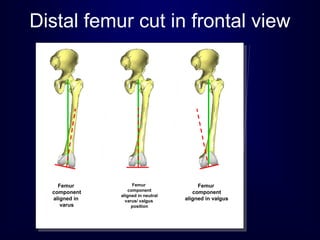
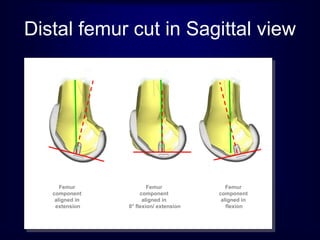
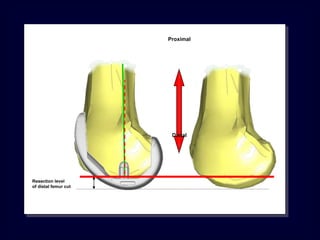
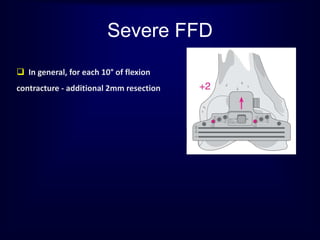
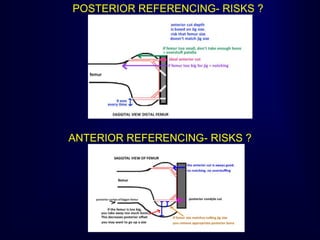
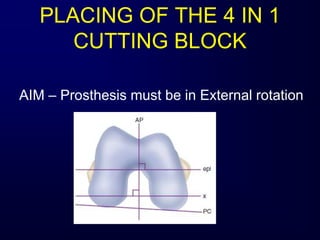
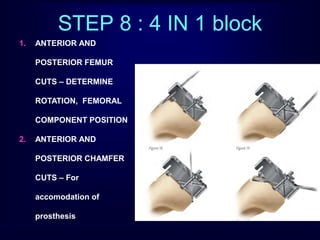
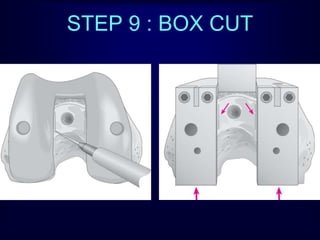
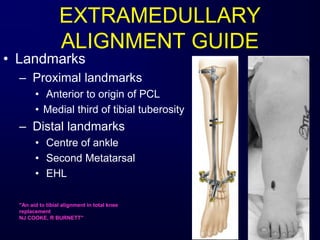
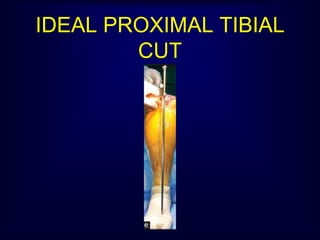
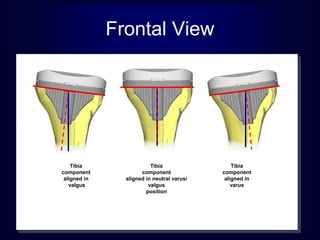
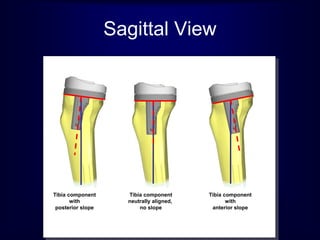
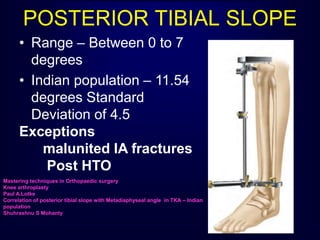
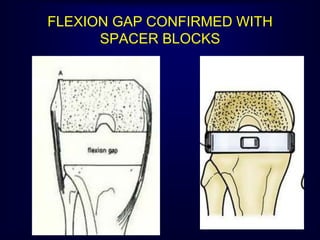
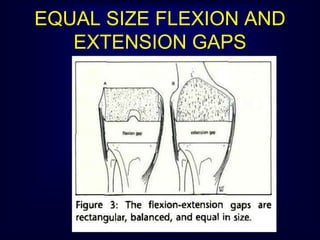
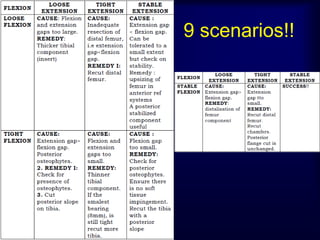
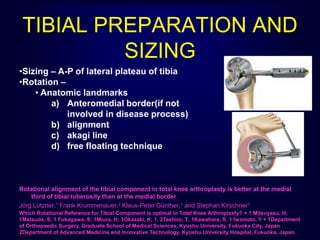
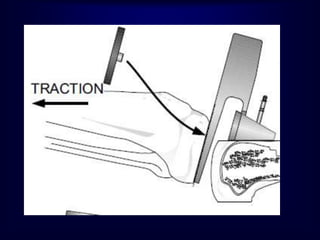
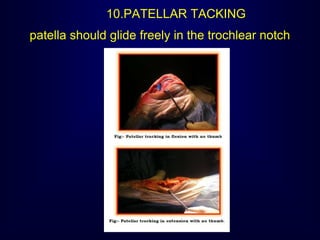
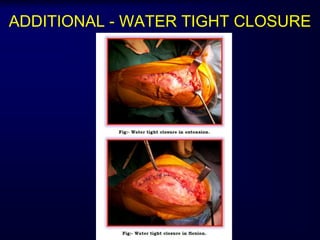
3. Key steps like distal femoral cuts, flexion and extension gap balancing, and tibial rotation and slope are explained. Ten commandments for optimal TKA outcomes are also listed.