Downloaded 895 times
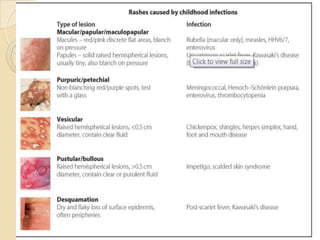
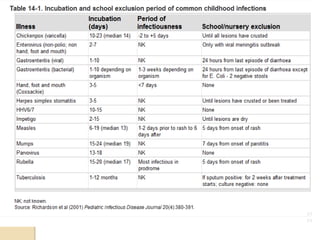
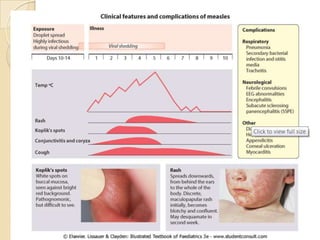


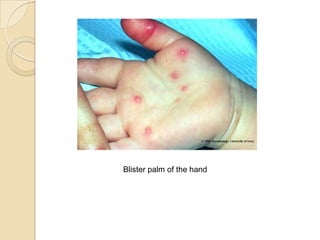
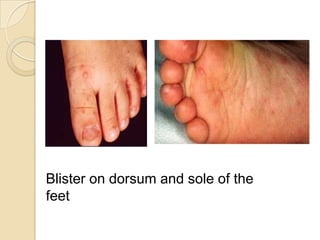


This document discusses diseases that present with fever and rash, focusing on measles, rubella, and hand, foot, and mouth disease. It describes the etiology, symptoms, diagnosis, and treatment of each condition. Measles is caused by a specific RNA virus and presents with a maculopapular rash. Rubella rash appears as pinpoint lesions and is generally milder than measles. Hand, foot, and mouth disease is common in children under 10 and caused by intestinal viruses, presenting with sores in the mouth and a non-itchy rash on the hands and feet.


























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










