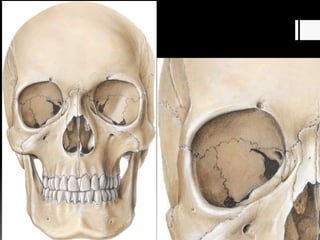
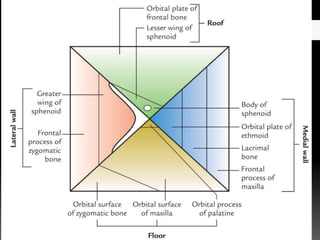
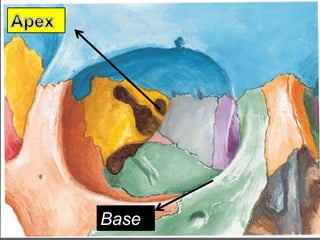
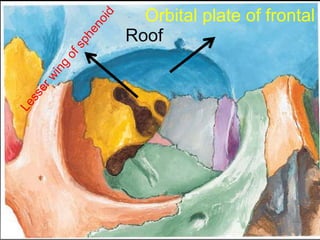
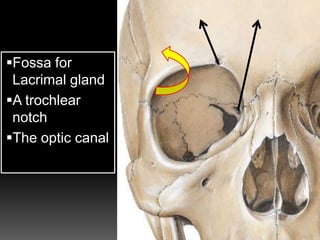
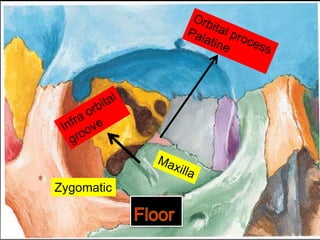
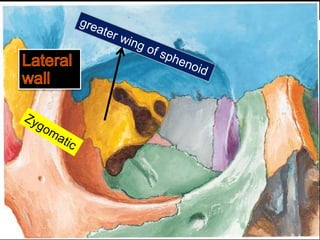
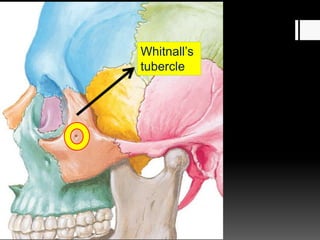
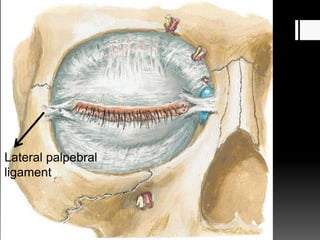
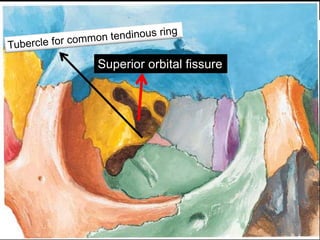
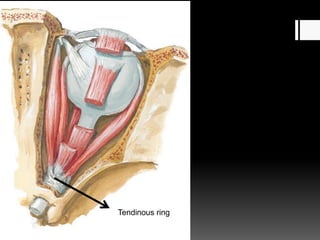
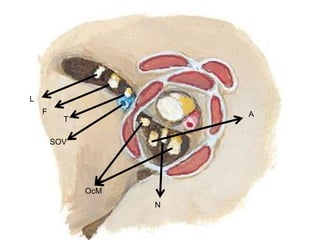
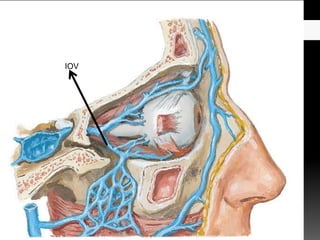
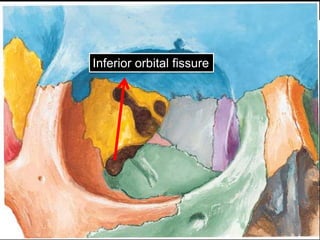
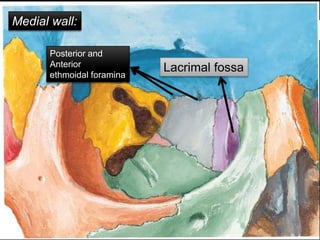
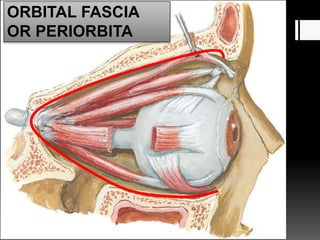
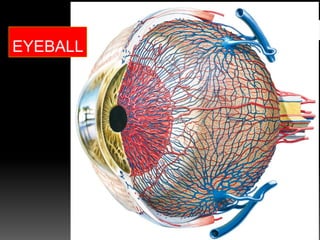
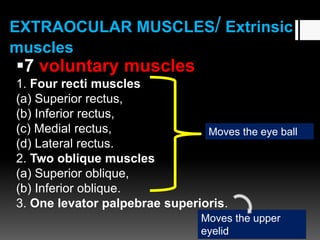
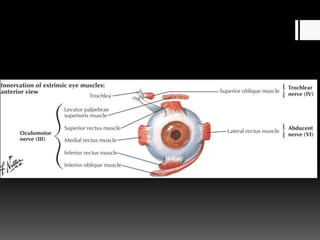
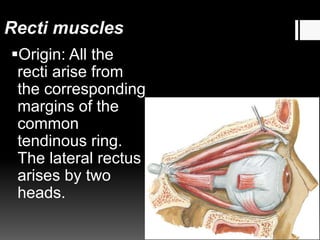
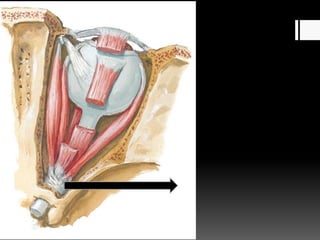
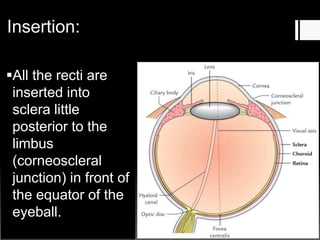
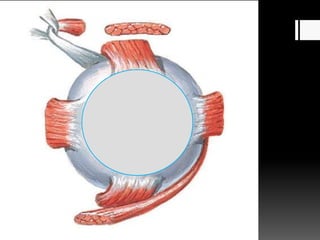
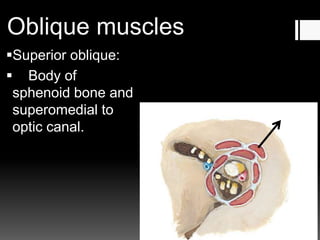
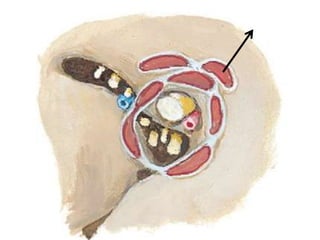
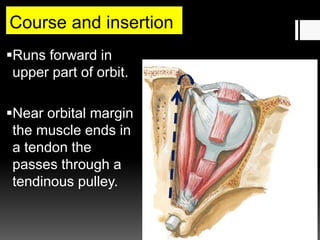
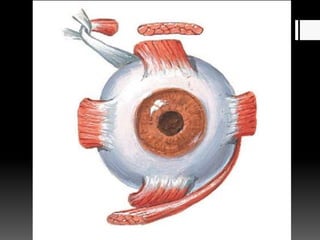
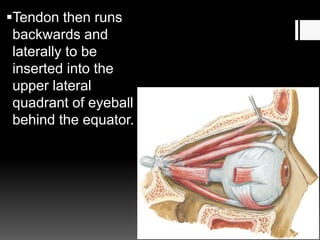
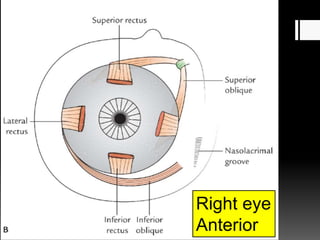
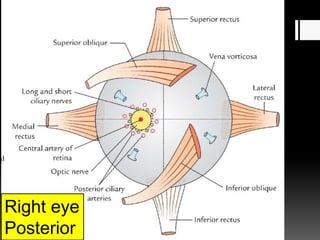
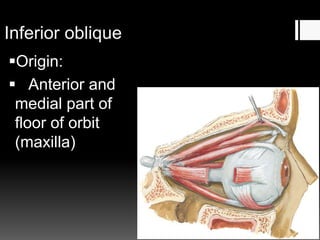
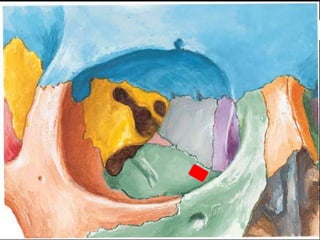
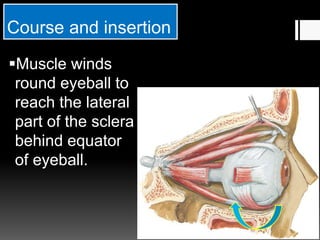
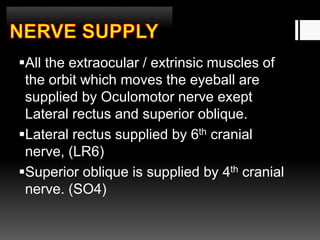
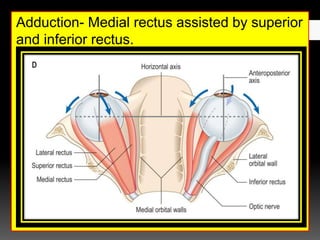
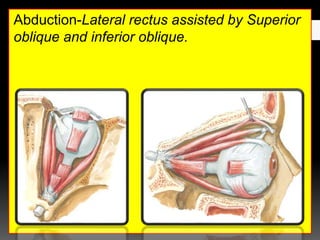
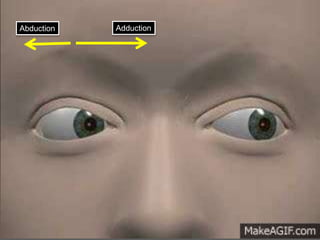
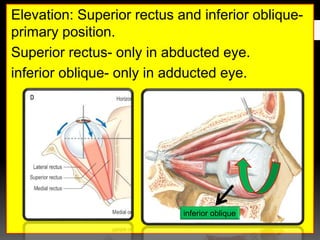
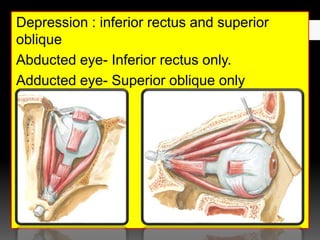
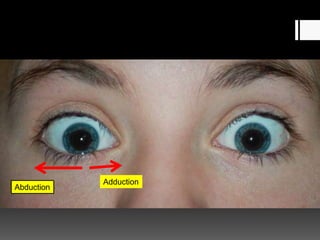
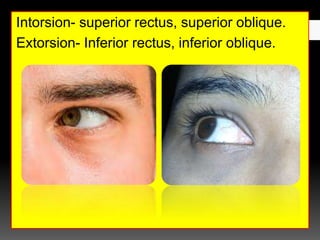
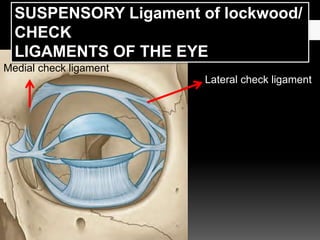
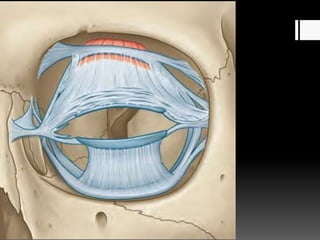
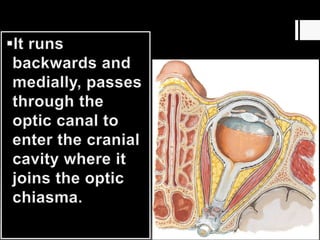
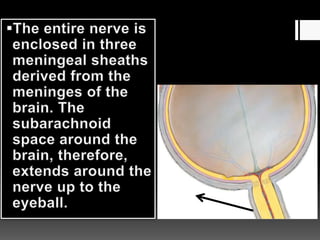
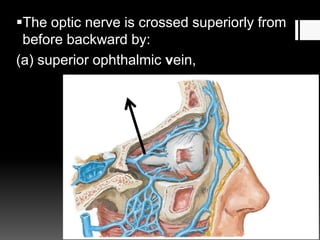
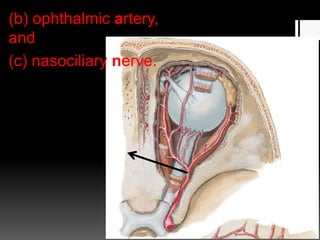
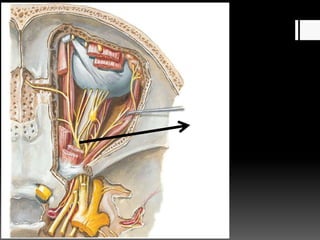
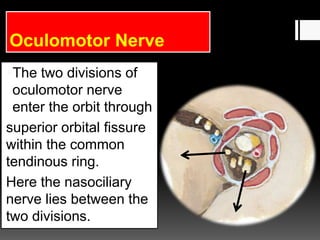
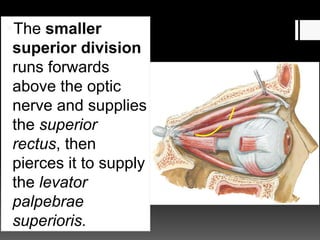
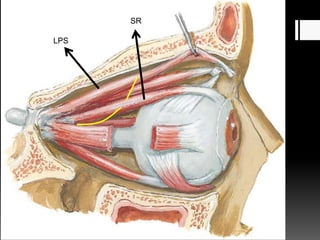
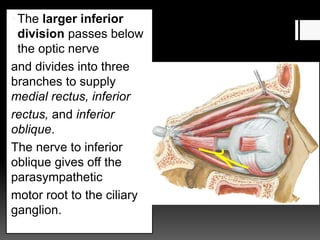
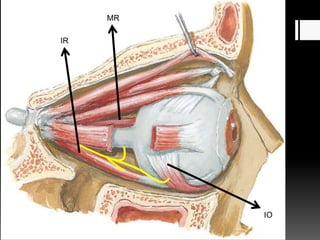
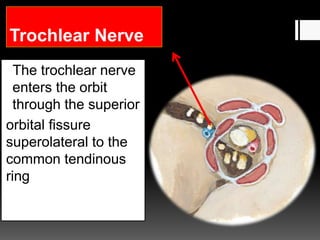
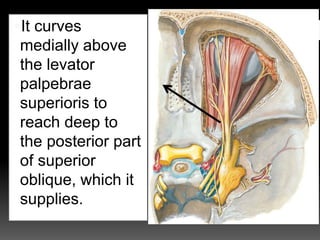
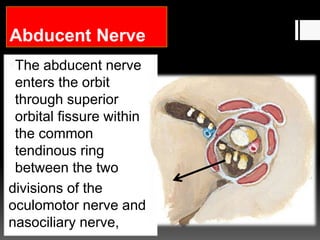
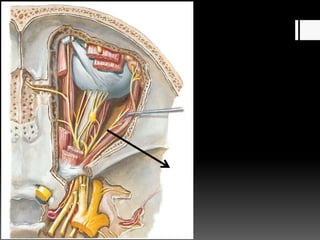
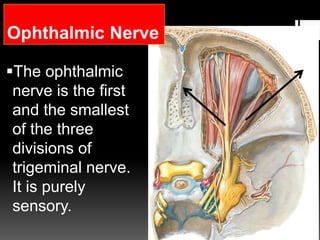
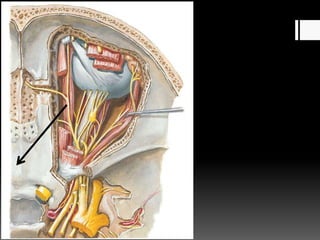
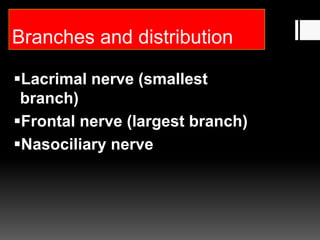
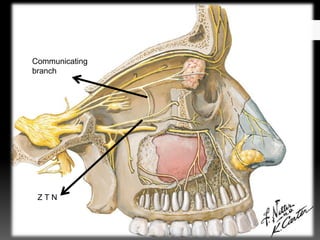
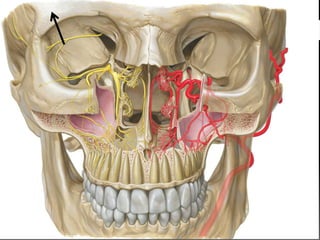
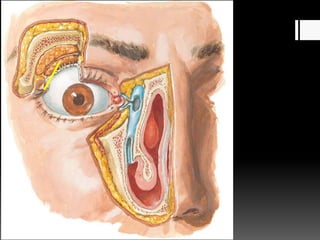
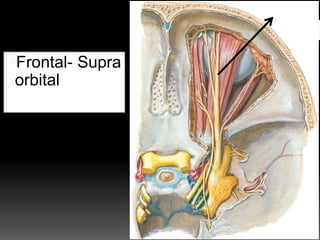
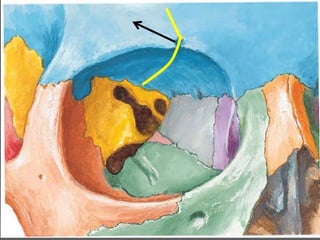
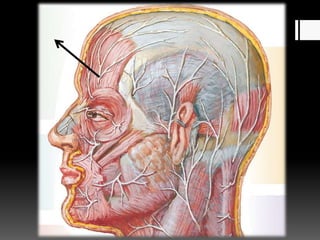
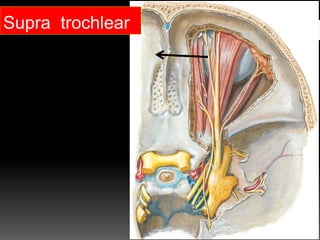
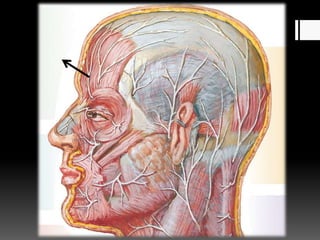
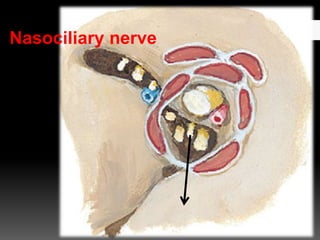
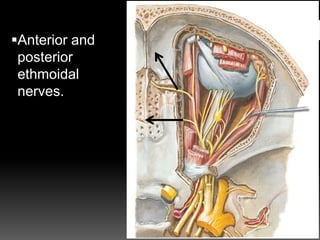
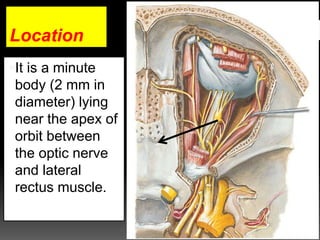
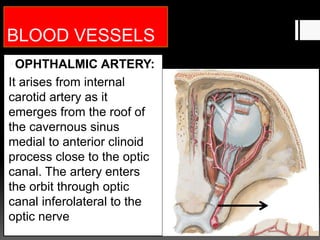
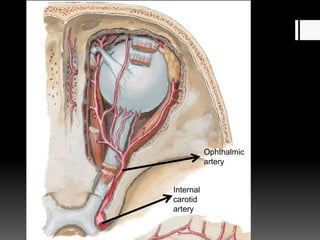
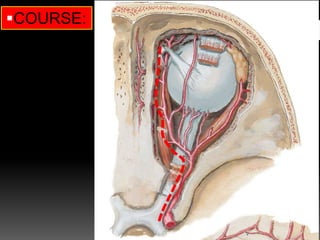
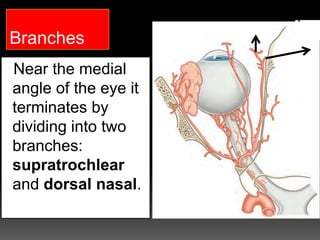
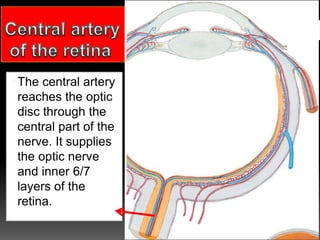
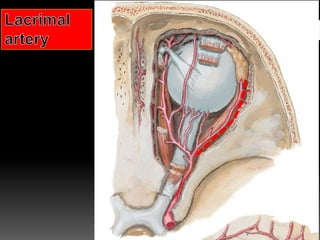
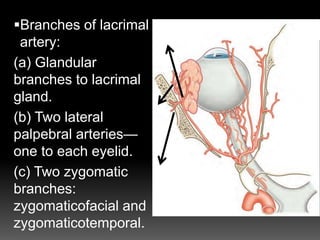
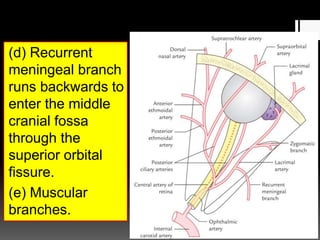
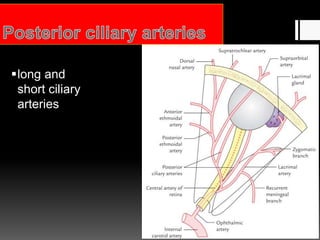
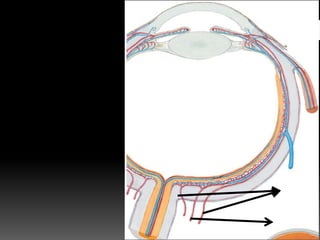
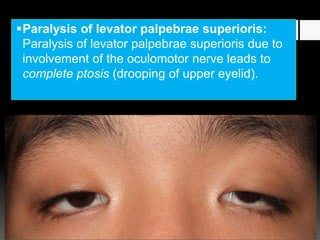
The document describes the anatomy of the orbit and its contents. It discusses the bones that form the boundaries of the orbit, including the roof, floor, lateral wall, and medial wall. It then describes the structures contained within the orbit, including the extraocular muscles, nerves, blood vessels, lacrimal gland, and orbital fat. It provides details on the origins, insertions, innervation and actions of each extraocular muscle. It also discusses the clinical implications of injuries or disorders that may affect structures in the orbit.