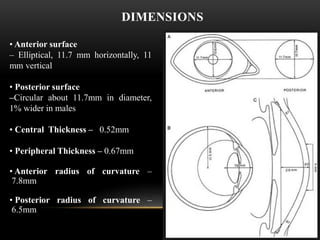
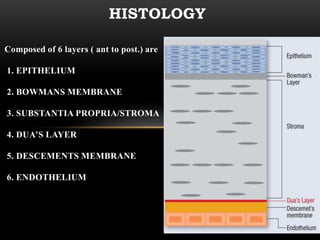
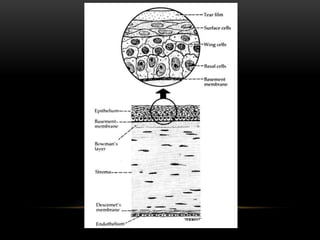


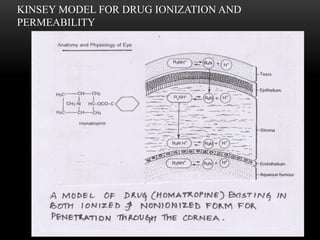
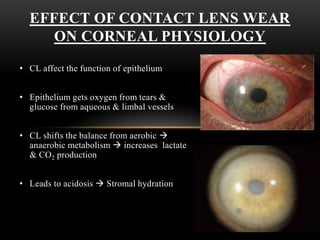


This document provides information on the anatomy and physiology of the cornea. It describes the layers of the cornea including the epithelium, Bowman's membrane, stroma, Dua's layer, Descemet's membrane, and endothelium. It discusses the transparency of the cornea, metabolic processes, drug permeability, wound healing, and the effects of contact lens wear on corneal physiology. The cornea has several specialized functions including refracting light and protecting the interior of the eye.

























































































