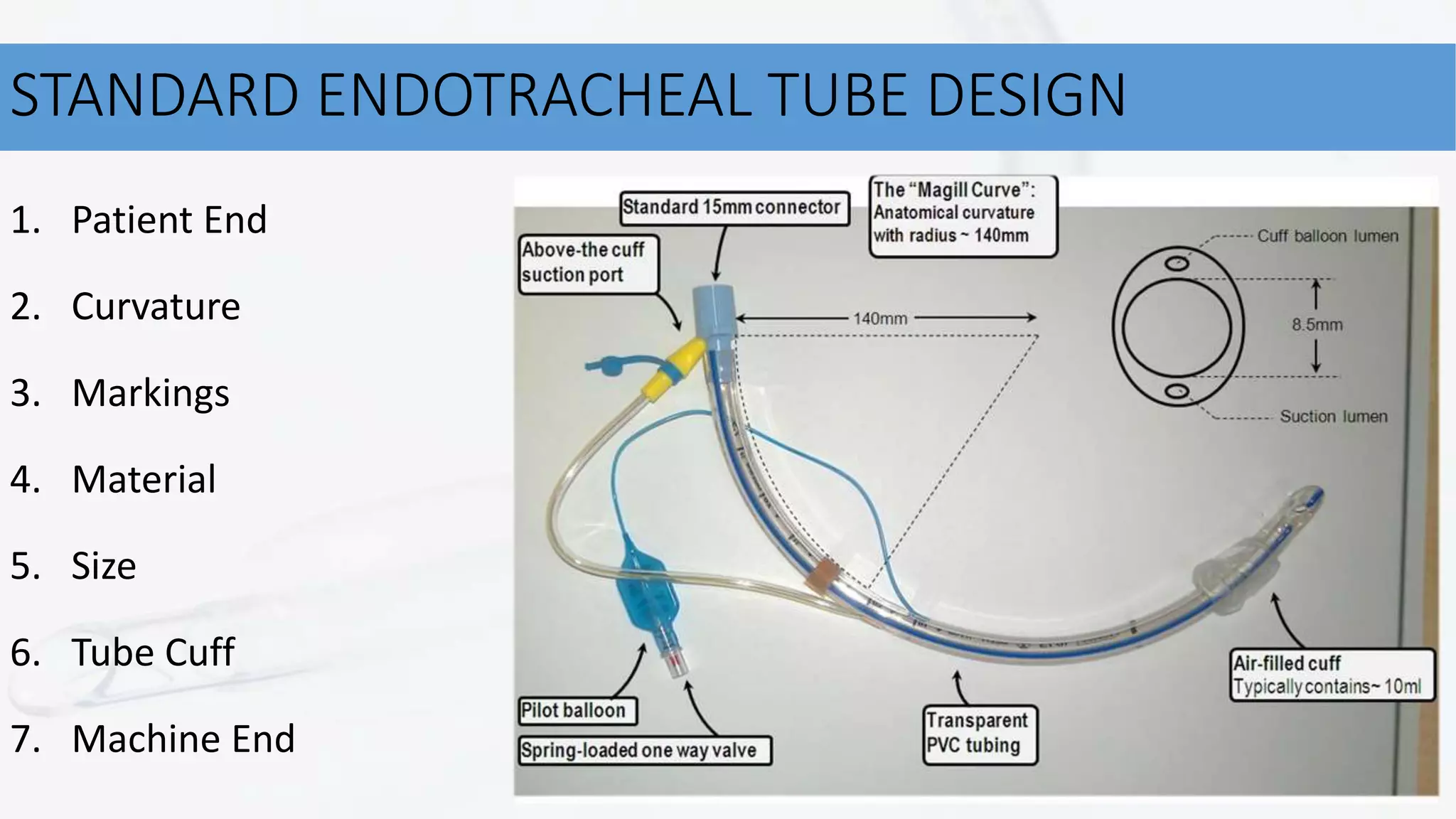
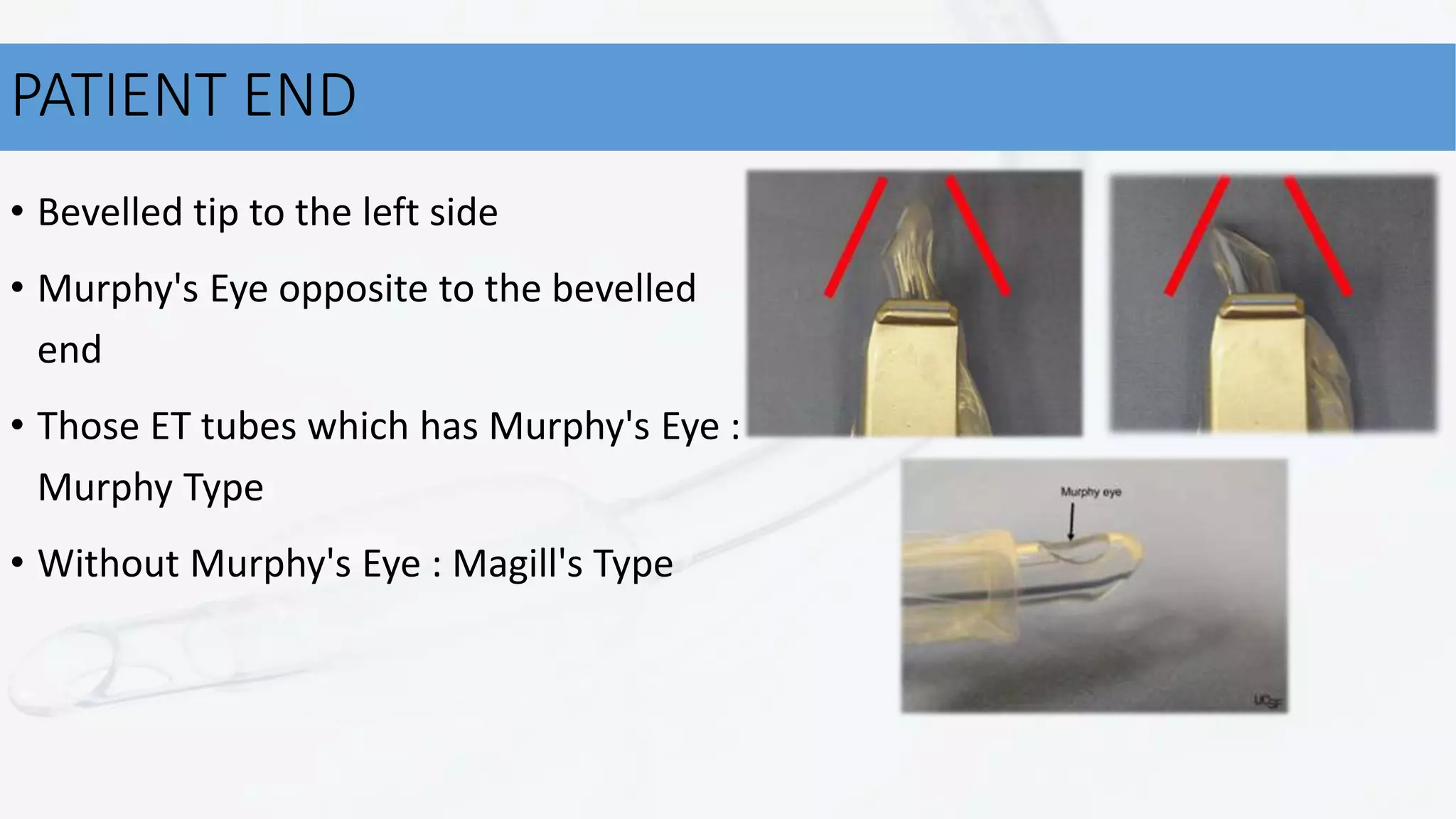
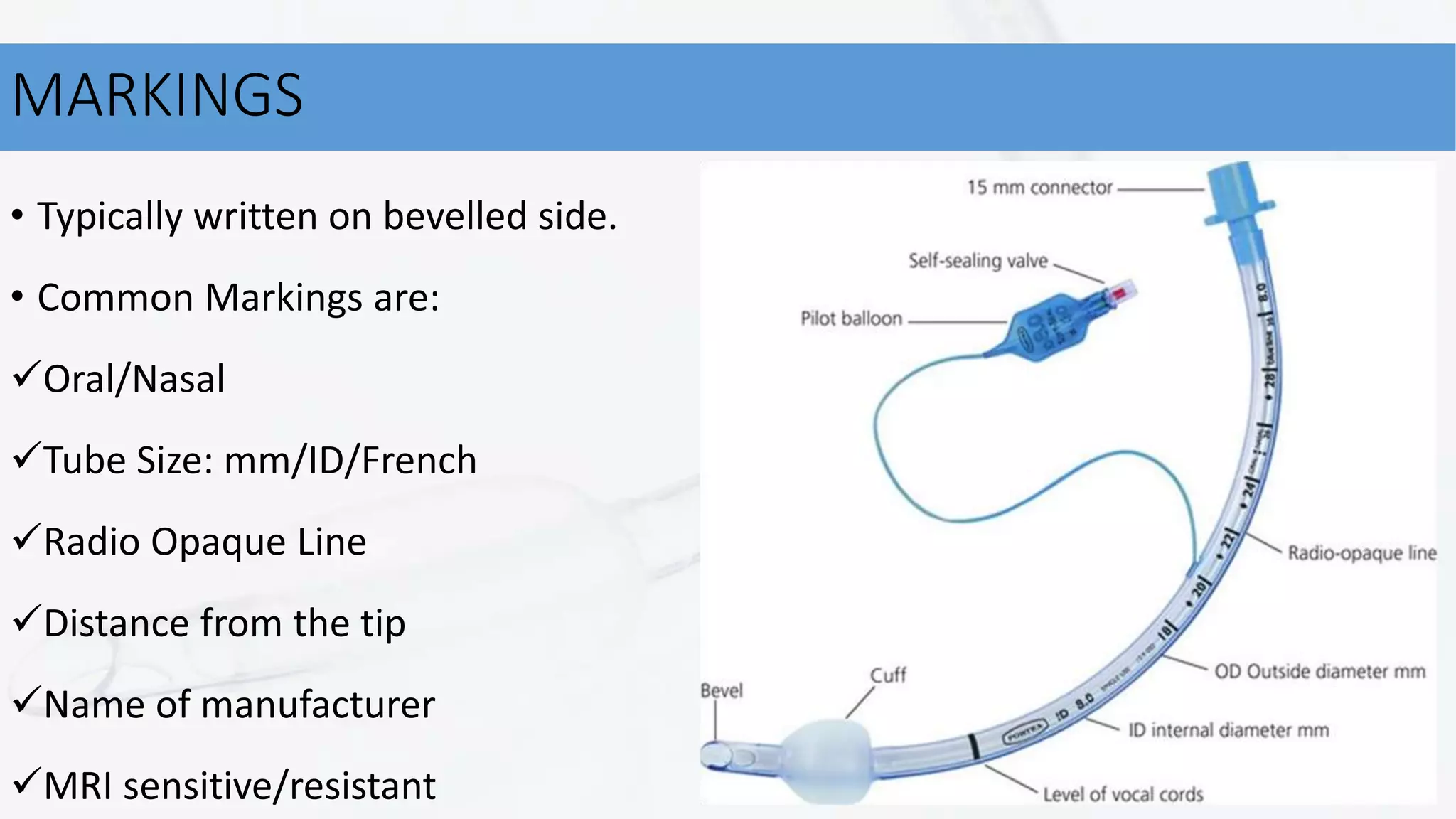
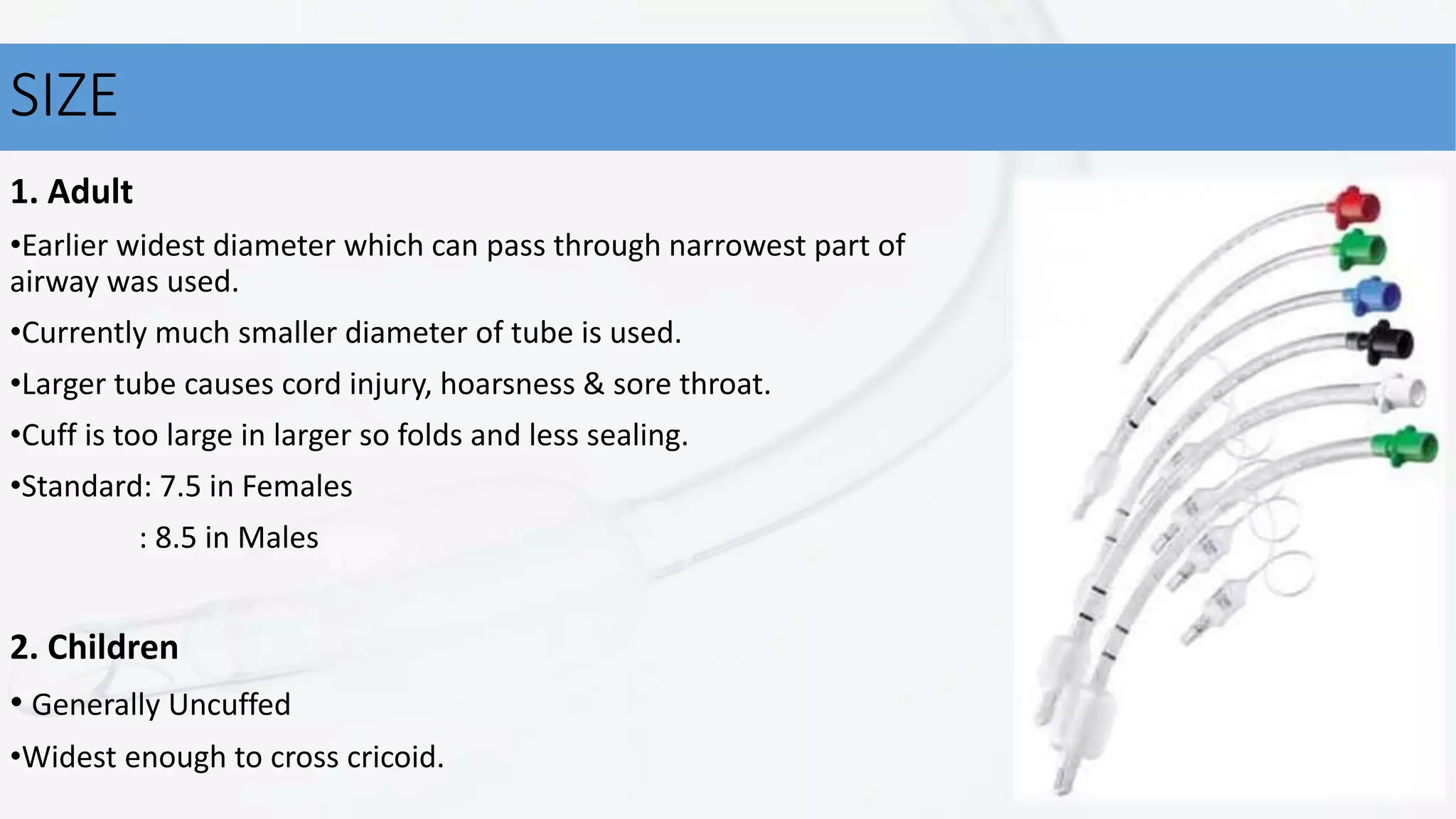
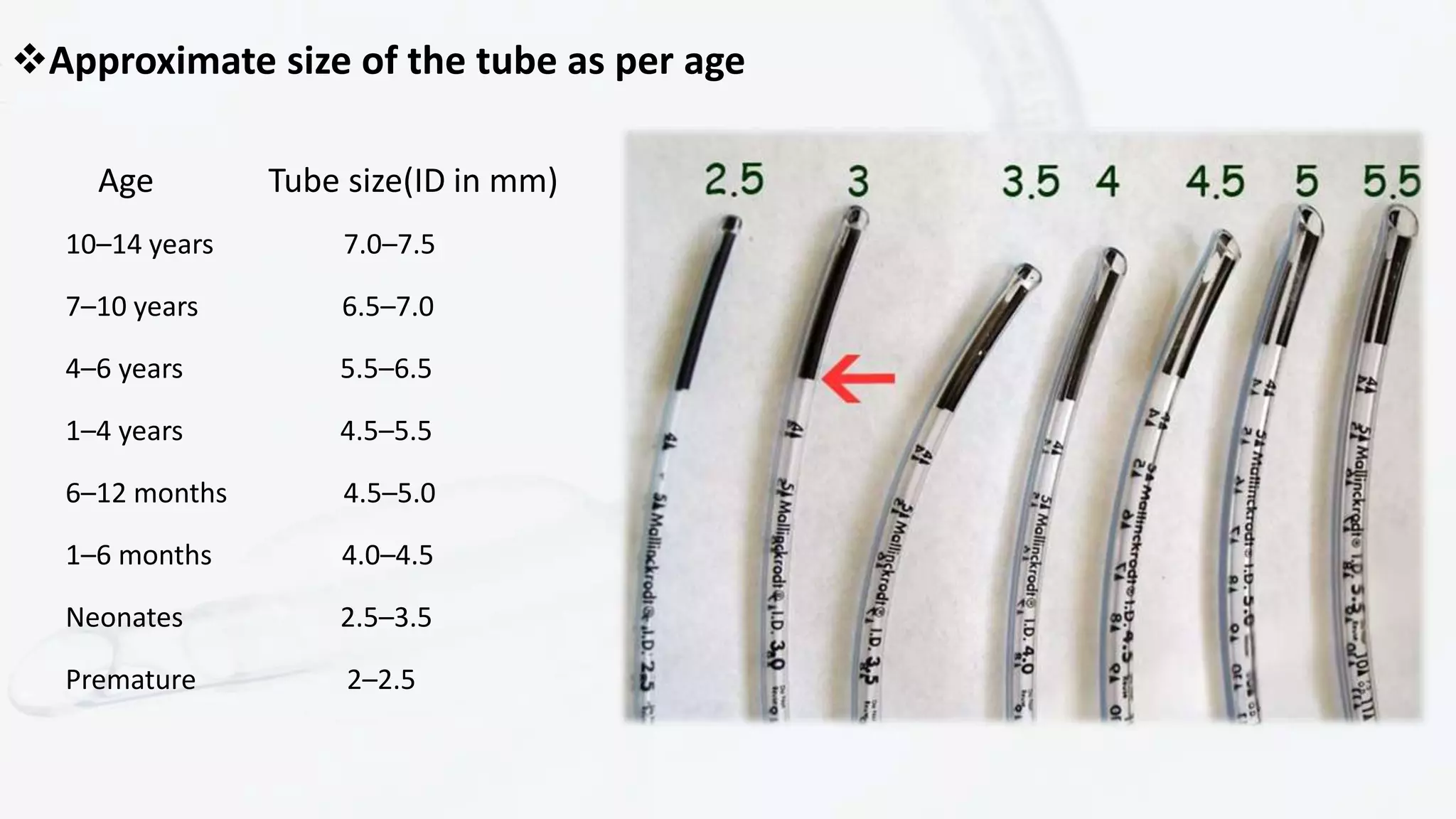
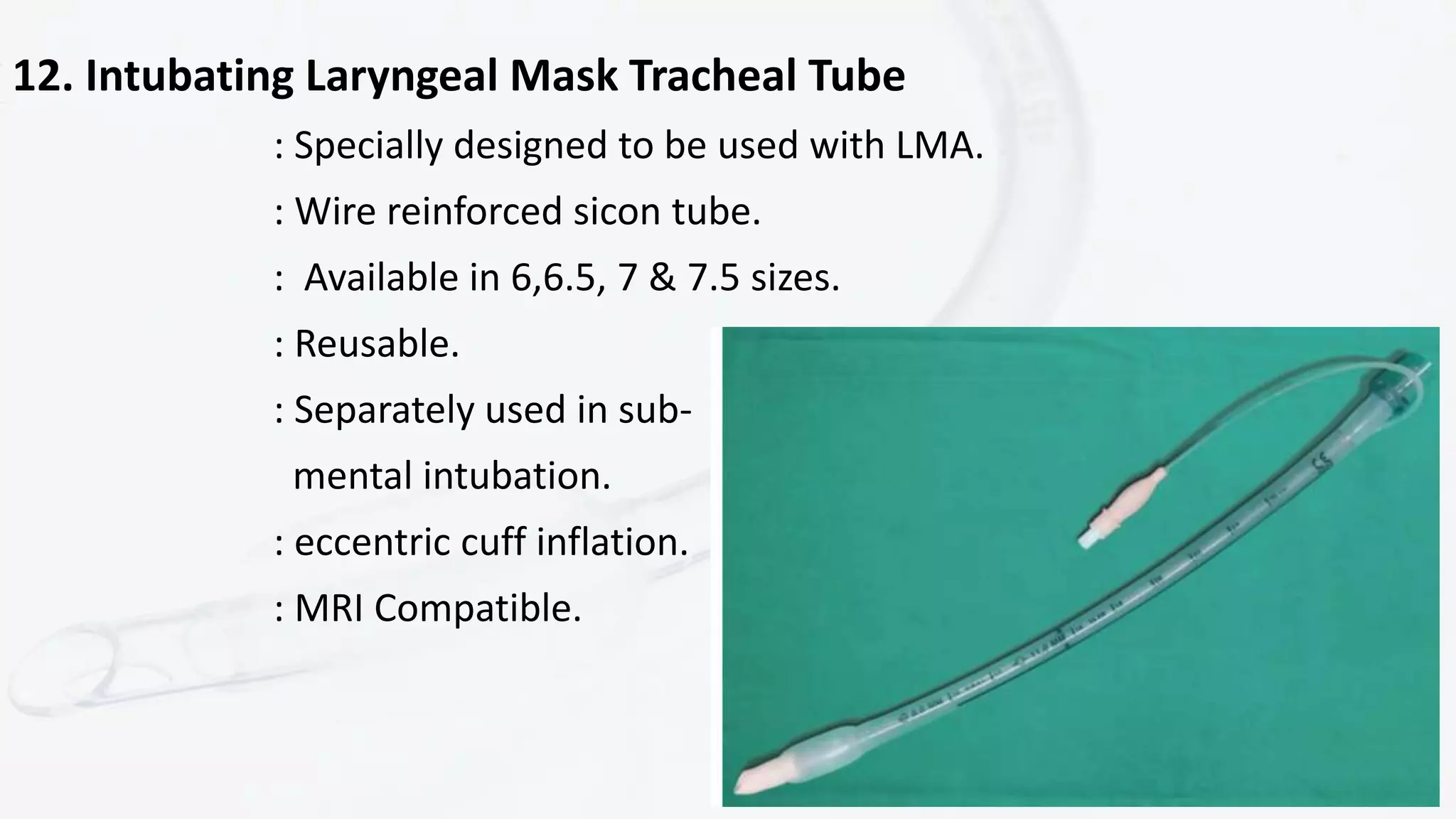
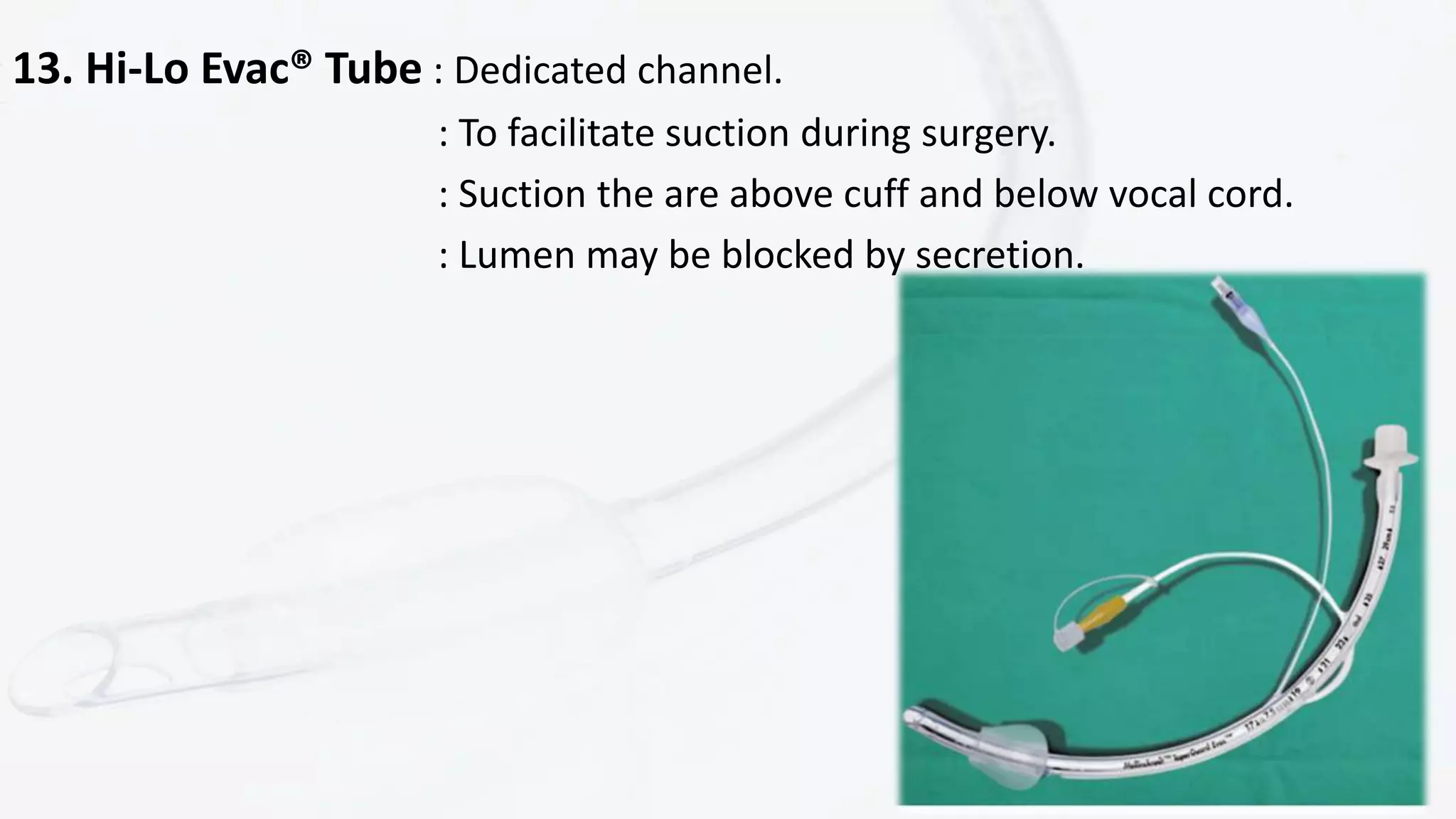
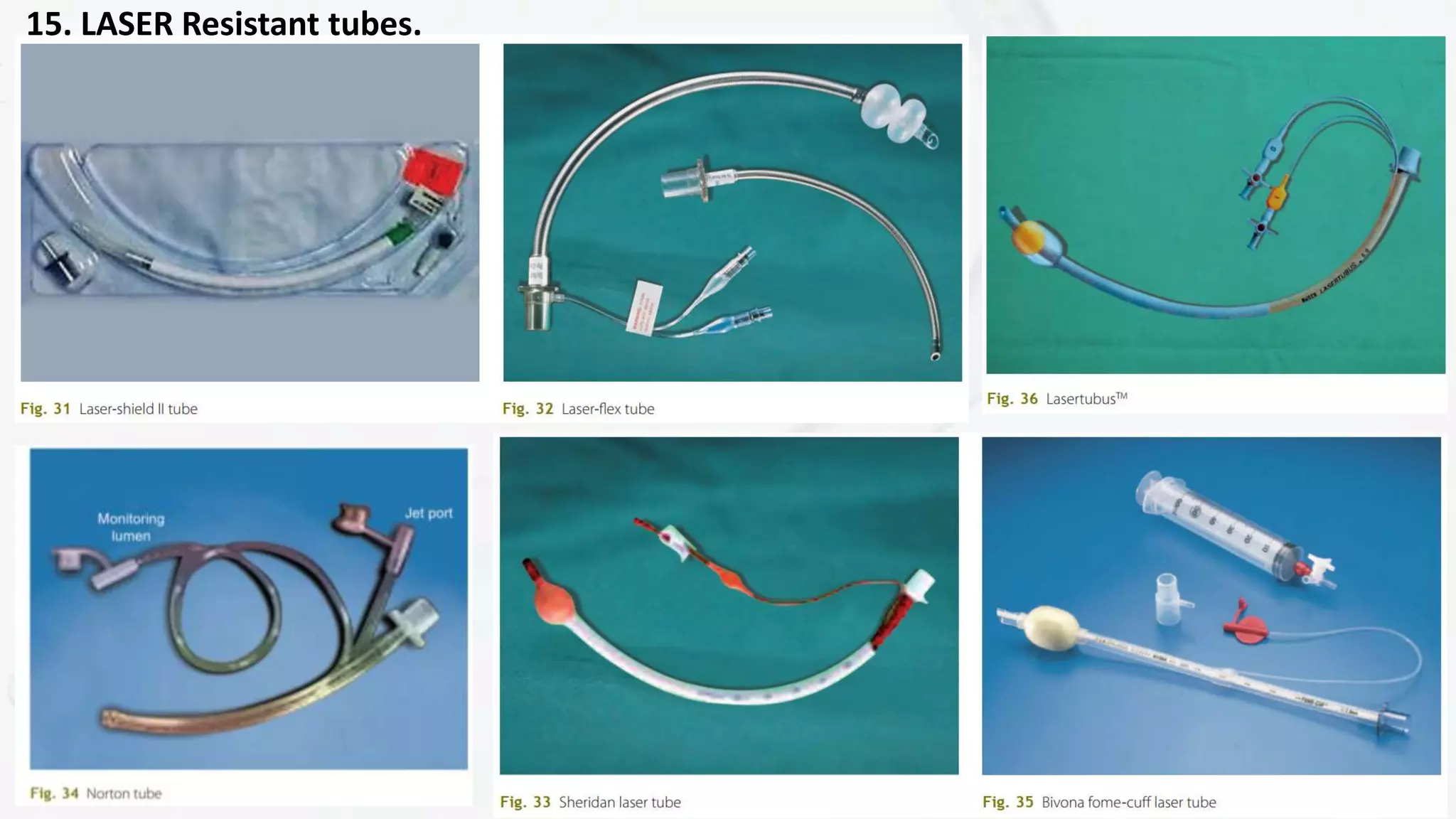
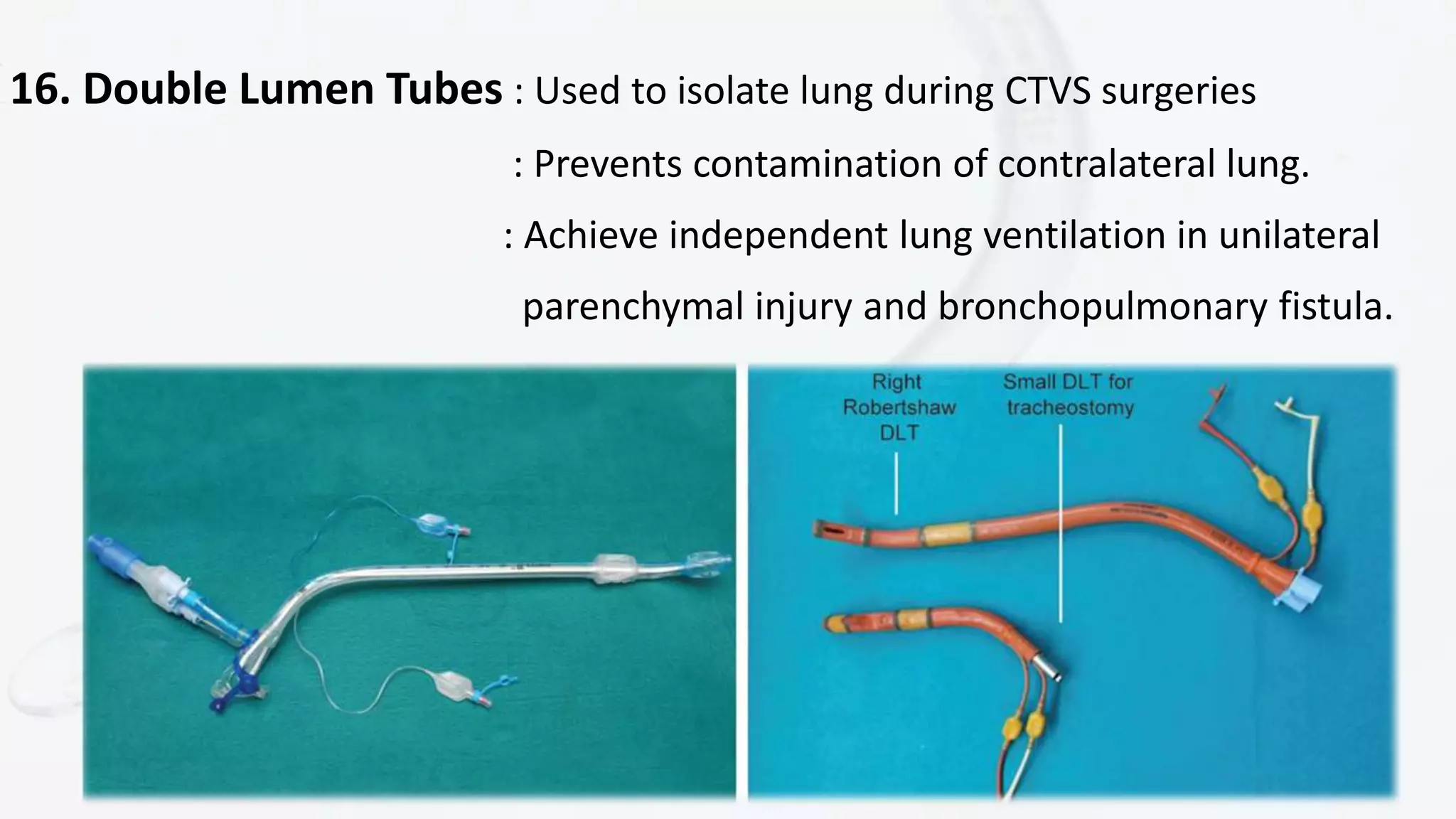
This document discusses different types of endotracheal tubes. It begins with a brief history of endotracheal intubation and then describes the standard design features of endotracheal tubes including the patient end, curvature, markings, materials, sizes, tube cuffs, and machine end. It then discusses several speciality endotracheal tubes designed for specific purposes like neonatal resuscitation, microlaryngeal surgeries, nasal intubation, and monitoring electrodes during laryngeal surgery. In total, over 15 different endotracheal tube varieties are outlined.