

























![PPLAT
F
PEEP
RR
RAW
VT
MECHANICAL
POWER
• P= TV*ERS + RAW*F + PEEP
EQUATION
OF MOTION
• 1/2*VT*VT*ERS+ VT*RAW*F +
VT*PEEP
EBREATH
• 0.098*RR[VT
2 {1/2*ERS +
RR*(1+I:E)/(60*I:E)*RAW} + VT*PEEP]
POWERRS
MECHANICAL POWER](https://image.slidesharecdn.com/mathematicsofpulmonarymechanics-171128131955/75/Mathematics-of-pulmonary-mechanics-40-2048.jpg)




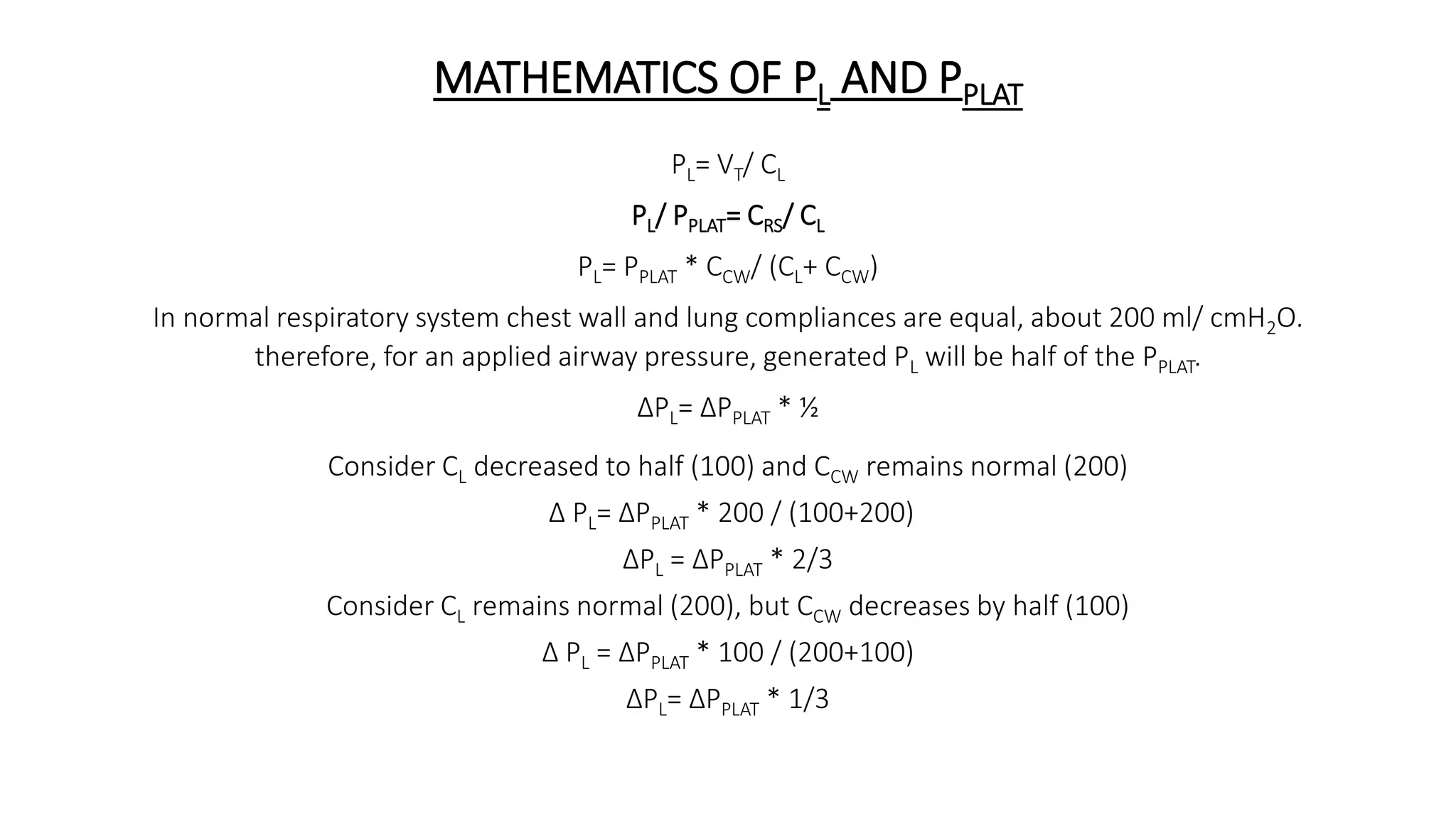
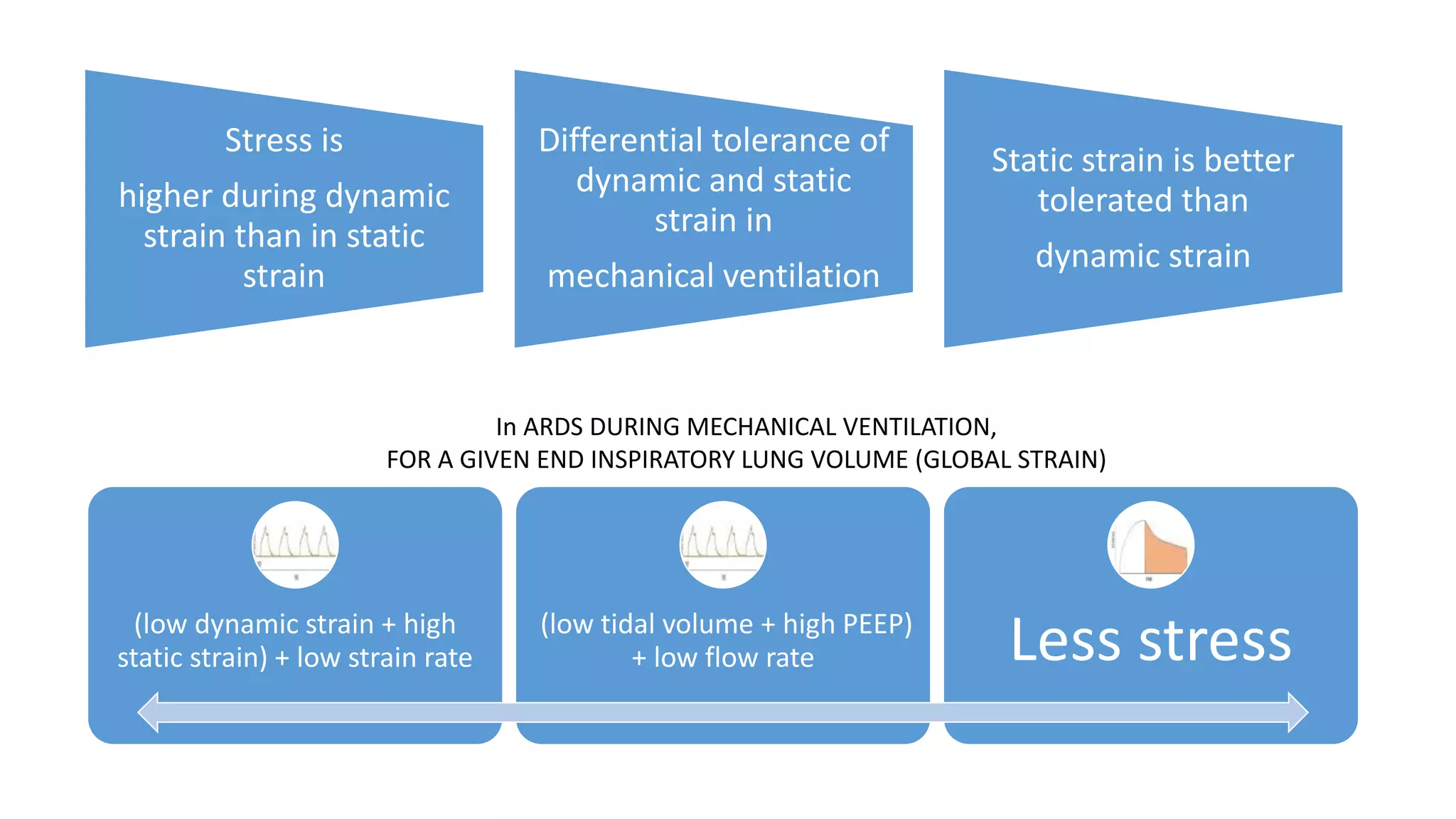
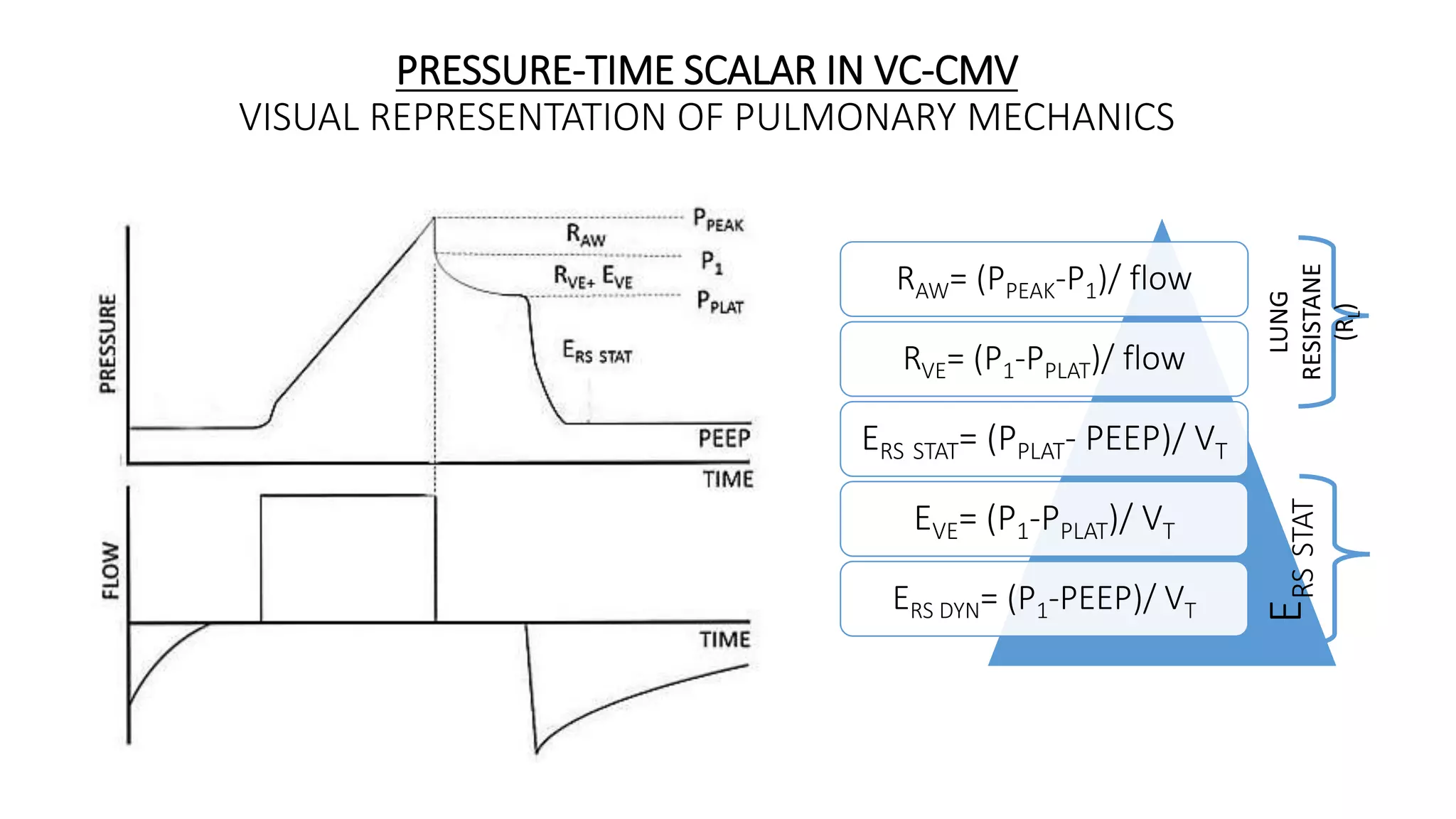
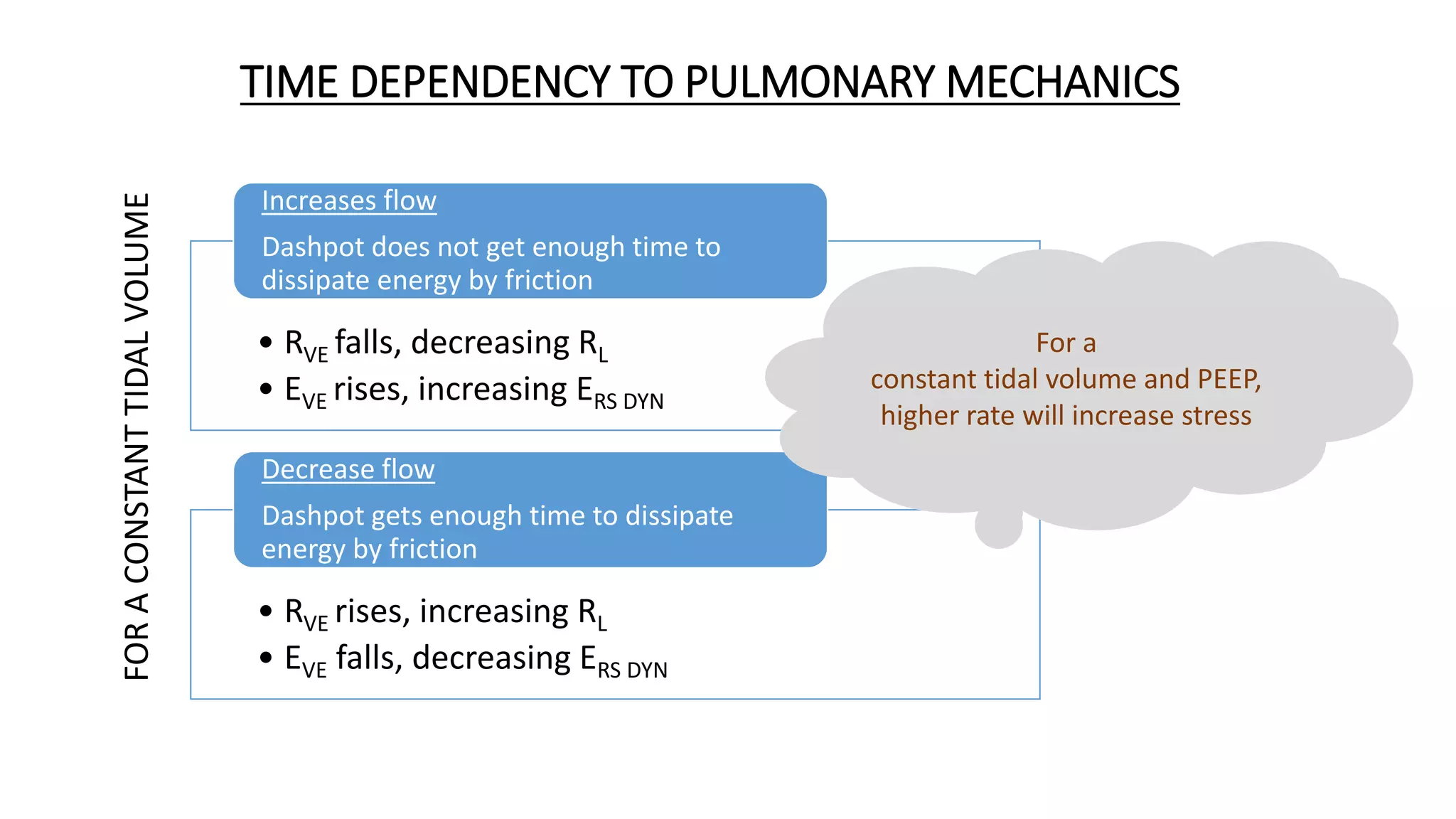
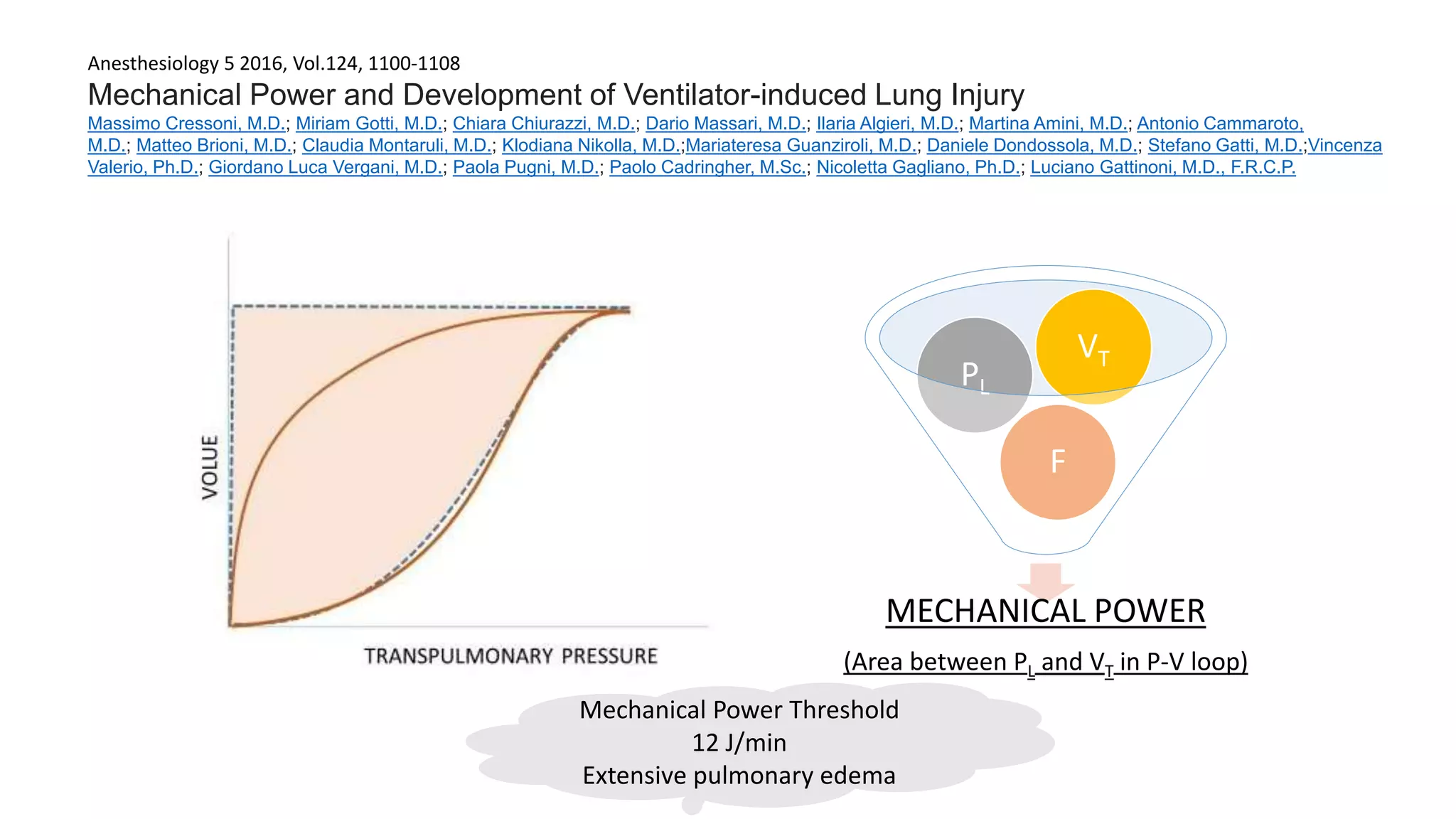
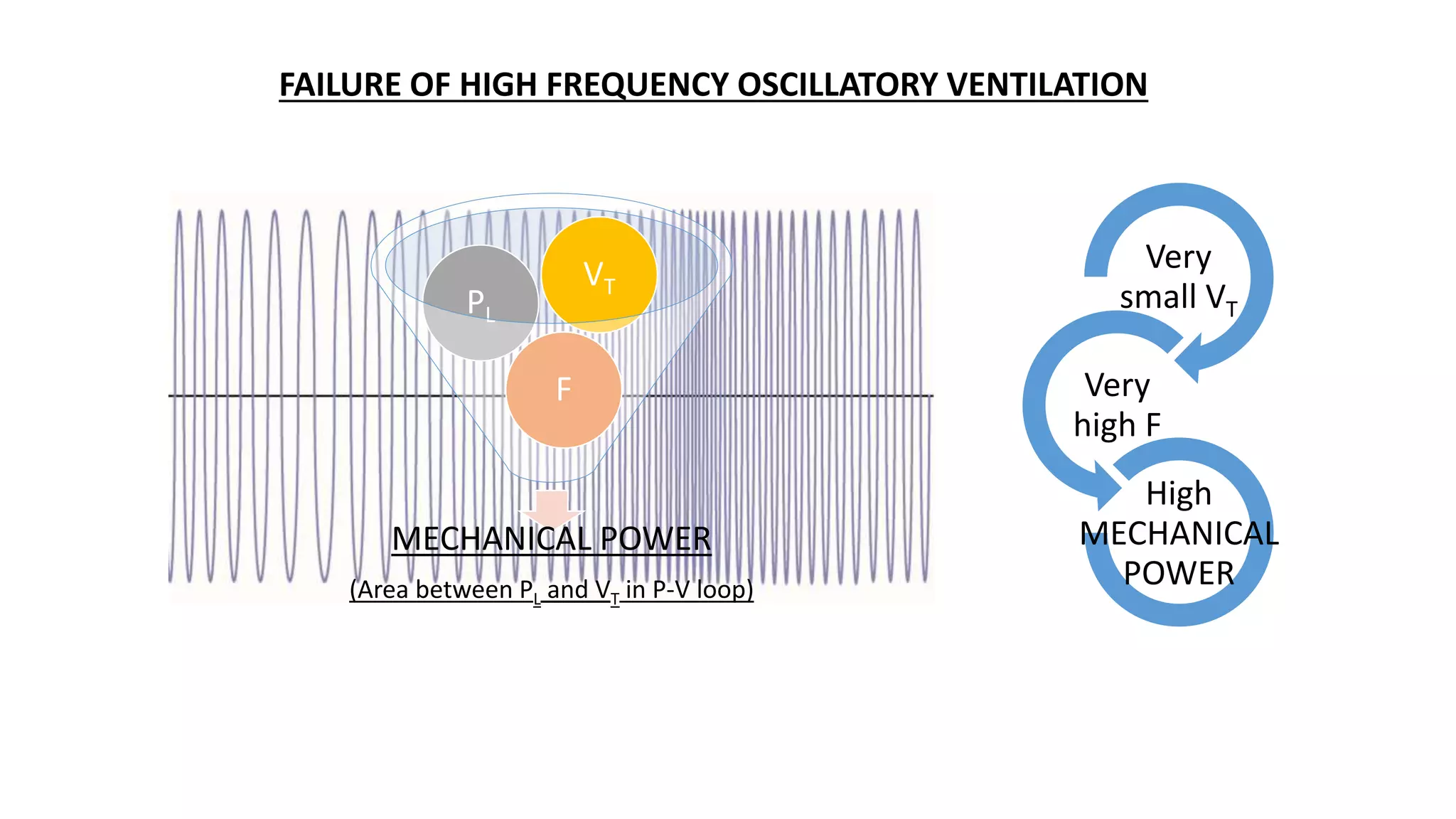
1. Tidal volume based on ideal body weight does not accurately represent lung strain which varies with severity of ARDS. 2. Plateau pressure is not a reliable surrogate for lung stress as its relationship to transpulmonary pressure depends on lung and chest wall compliance. 3. Respiratory frequency and flow influence pulmonary mechanics in a time-dependent manner, contributing to mechanical power delivered and ventilator-induced lung injury (VILI).























































































