This document provides a comprehensive overview of mechanical ventilation, including its purposes, techniques, and nursing responsibilities. It covers mechanical and non-invasive ventilation modes, ventilator parameters, indications for use, potential complications, and nursing care practices. The document emphasizes the importance of monitoring patients, preventing infections, and ensuring proper nutrition while on ventilation.



![VENTILATOR PARAMETERS
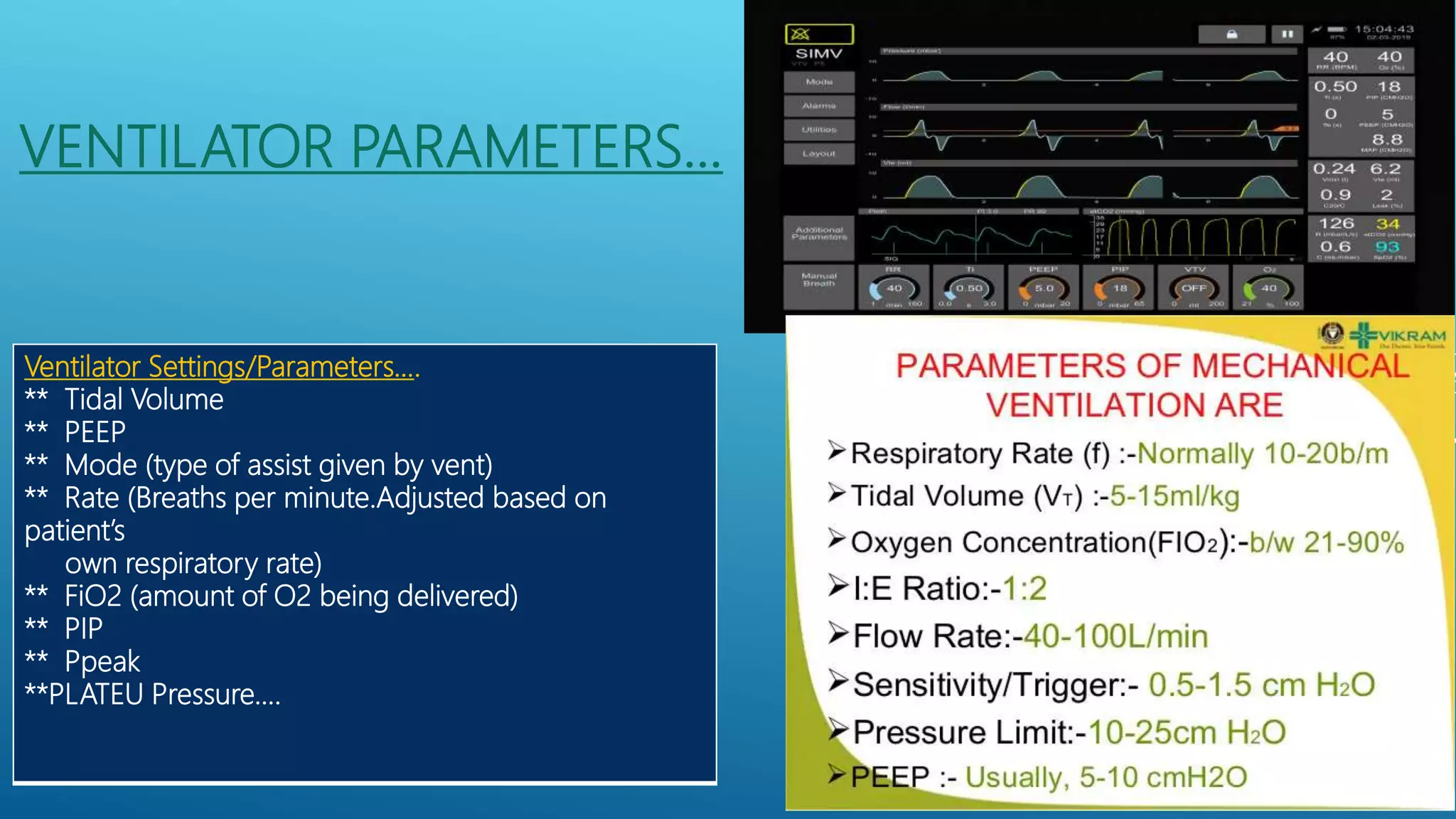
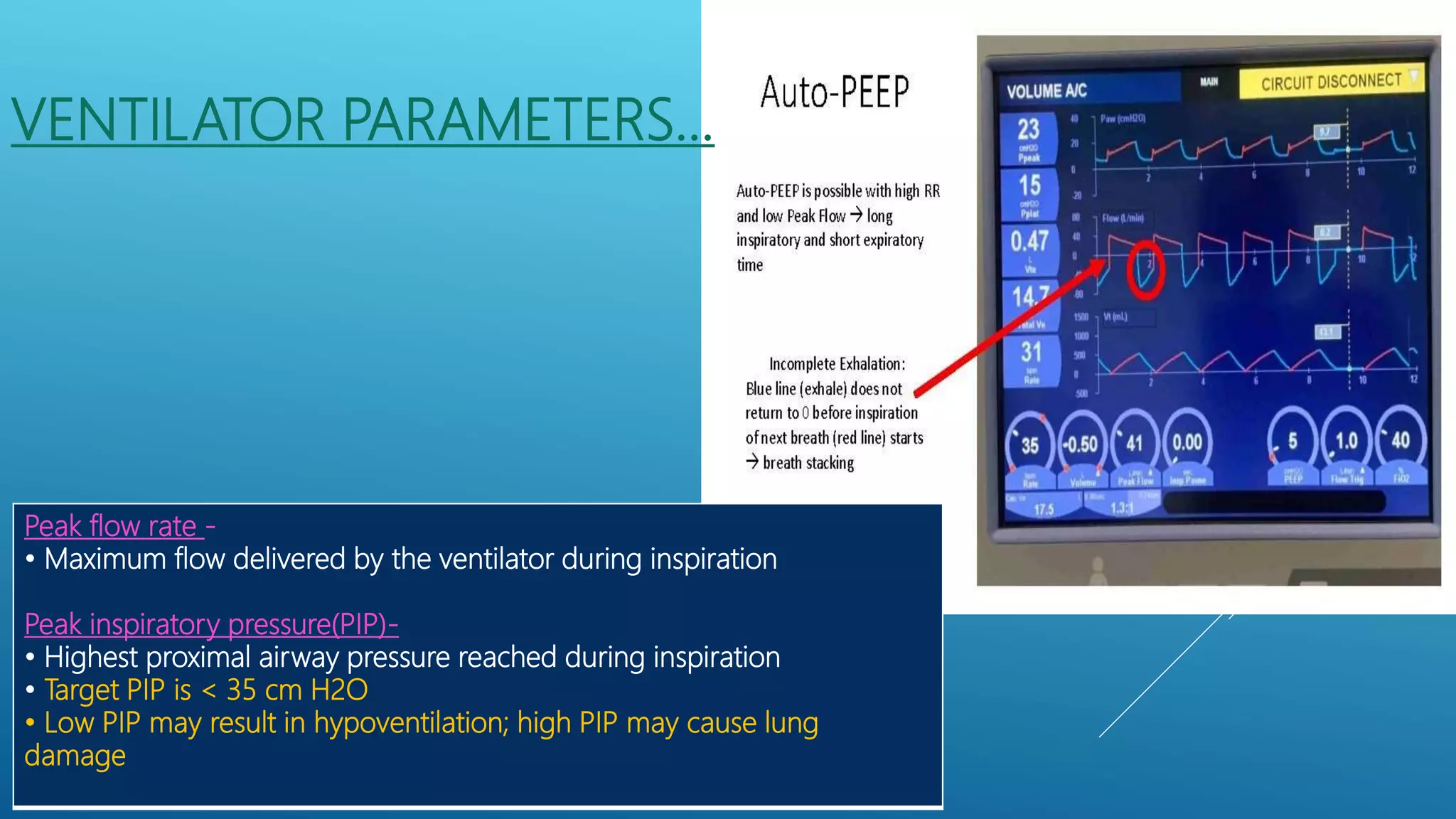
Tidal volume (VT)
Normally;6-8 mL/kg of ideal bodyweight [IBW] to preventbarotrauma)
VT means- Volume of gas exchanged with each breath
• A lower VT is indicated in patients with stiff, non-compliant
lungs
• Higher VT may cause tachycardia, decreased blood pressure
and lung injury
LOW TIDAL VOLUME VENTILATION
Trigger
Breaths can be triggered by:
Timer (ventilator-initiated breaths); occur at the set
respiratory rate or frequency
Patient effort (patient-initiated breaths); occur when the
patient causes sufficient change in either the pressure or
flow in the circuit](https://image.slidesharecdn.com/mechanicalventilatorcommonmodesindicationsnursisngresponsibilitiesmurugesh2nd-210824153035/75/Mechanical-ventilator-common-modes-indications-nursing-responsibilities-12-2048.jpg)



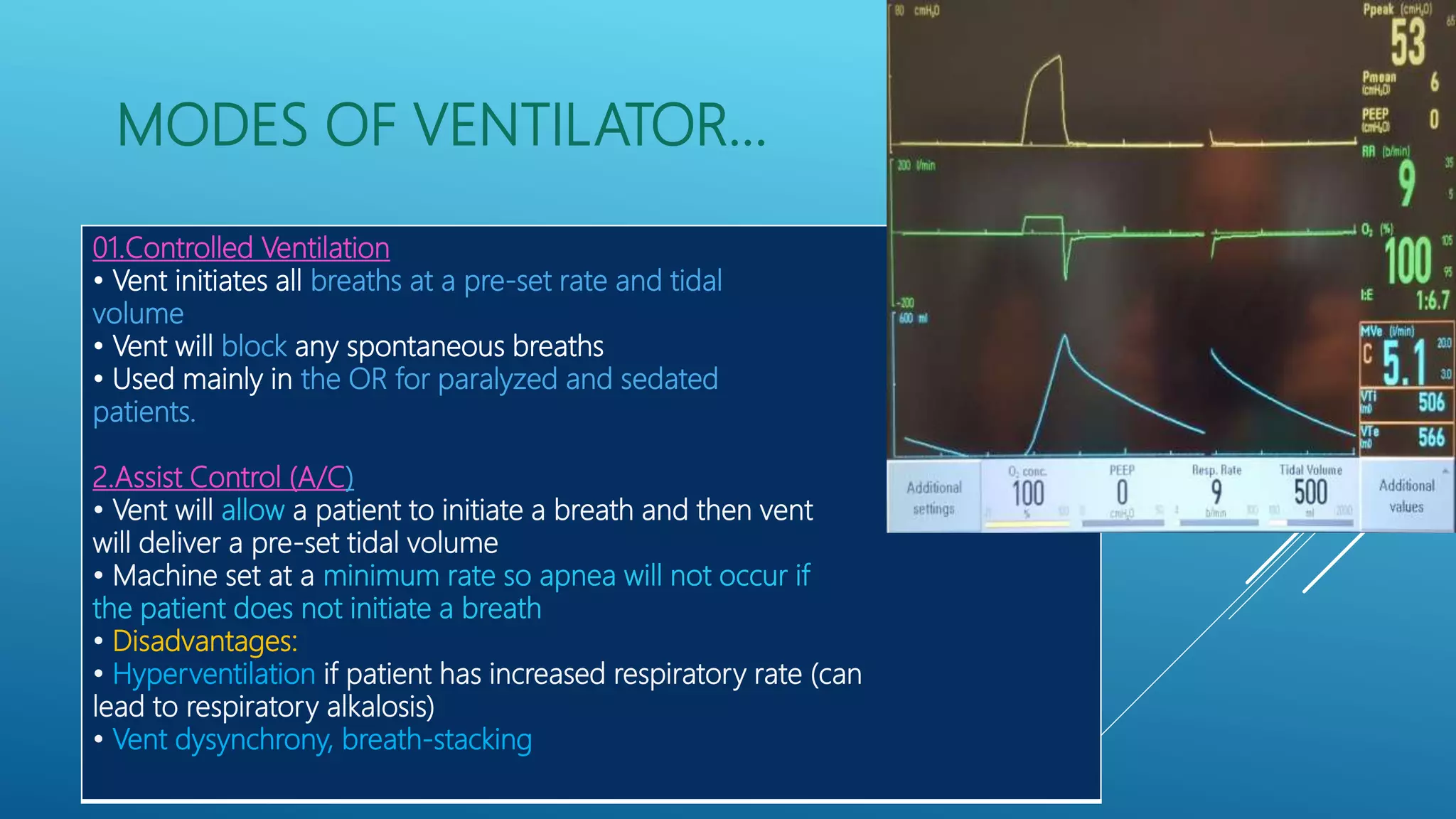



![PRVC MODE OUTCOMES…..
EXPECTED OUTCOMES or ADVANTAGES
• Risk of barotrauma is reduced.
• Ventilator alarms when pressure limit is reached.
• Patient’s ventilation and oxygenation status are improved as evidenced by ABG
values,
decreased FIO2, decreased work of breathing, and improved vital signs.
UNEXPECTED OUTCOMES OR DISADVANTAGES
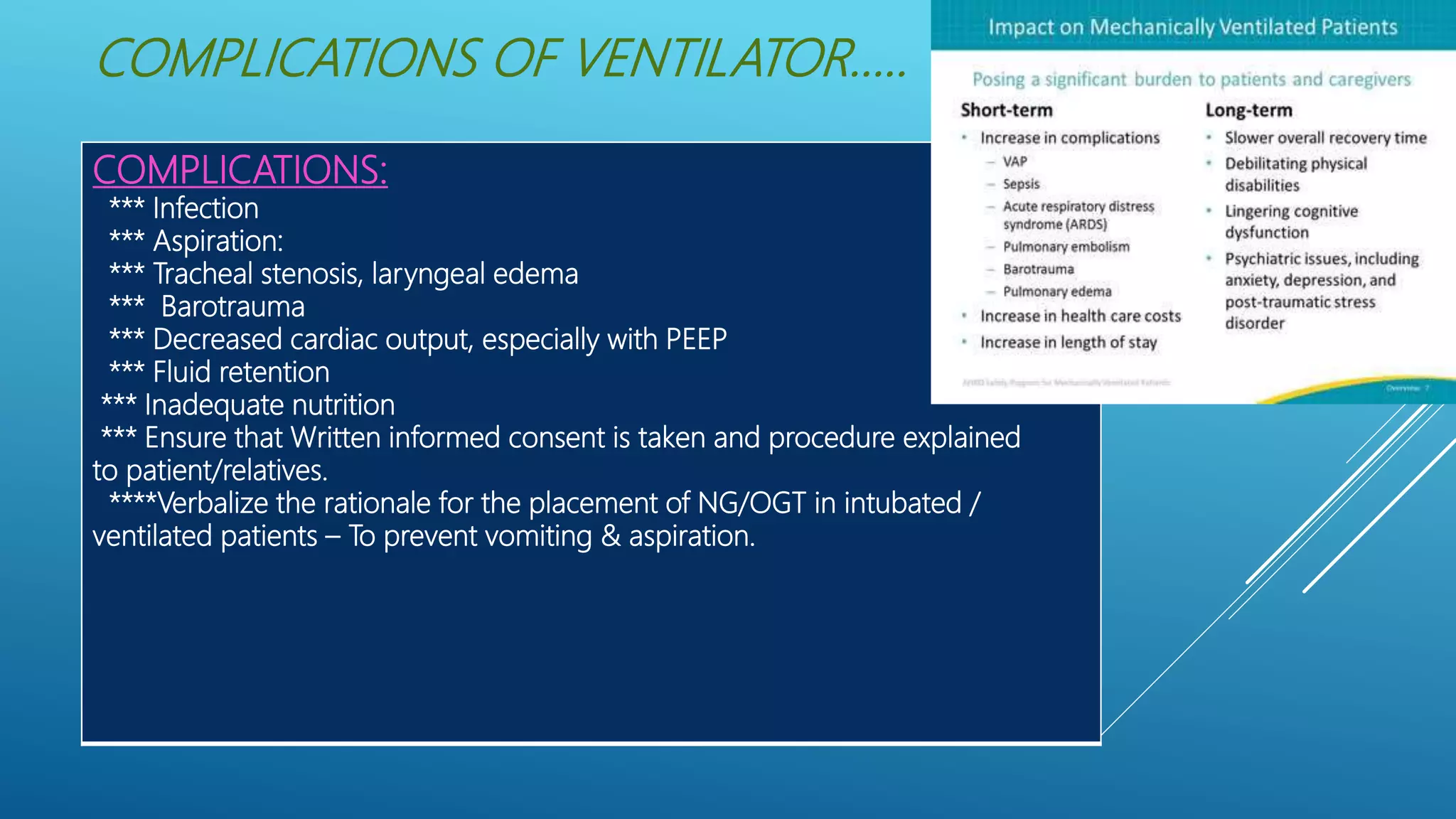
• Infection
• Hemodynamic compromise
• Complications associated with artificial airways (e.g., leaks, cuff rupture,
obstruction of endotracheal [ET] tube, pressure necrosis)
• Patient-ventilator asynchrony (e.g., auto-PEEP
, hyperventilation or
hypoventilation,
increased work of breathing, hyperoxygenation or hypo-oxygenation)
• High pressure reached before volume is delivered and set volume not delivered
to patient](https://image.slidesharecdn.com/mechanicalventilatorcommonmodesindicationsnursisngresponsibilitiesmurugesh2nd-210824153035/75/Mechanical-ventilator-common-modes-indications-nursing-responsibilities-20-2048.jpg)