Endotracheal intubation(EI) is often an emergency procedure that’s performed on
people who are unconscious or who can’t breathe on their own. endotracheal
intubation maintains an open airway and helps prevent suffocation.
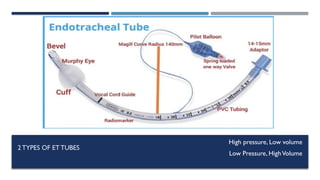
An endotracheal tube is a flexible plastic tube that is placed through the mouth into
the trachea (windpipe) to help a patient breathe.
3.
INDICATION
General surgery:With general anesthesia, the muscles of the body
including the diaphragm are paralyzed, and placing an endotracheal tube
allows the ventilator to do the work of breathing.
Foreign body removal
To protect the airway against aspiration: endotracheal tube may be placed
to help prevent the stomach contents from entering the airways.
4.
To visualizethe airway if an abnormality of the larynx, trachea, or
bronchi is suspected.
To support breathing if someone is having difficulty breathing due to
pneumonia, a pneumothorax, respiratory failure or unconsciousness due
to an overdose.
Some medical conditions (example Guillain-Barre syndrome) can result
in full or partial paralysis of the diaphragm and may require respiratory
support.
When sedation is required or higher concentration of oxygen needed.
Respiratory distress in premature babies often requires placement of an
endotracheal tube and mechanical ventilation.
5.
CONTRAINDICATION
Severe airwaytrauma that does not permit safe passage.
Cervical spine injury.
Mallampatic classification of class III / IV or other
determination of potential difficulty airway.
6.
EQUIPMENT FOR INTUBATION
Laryngoscope handle and blade (Macintosh and Miller blades)
Et tube (According to patient)
Stylet or Bougie
10 ml syringe to inflate cuff
Water soluble lubricant (Lignocaine jelly)
Stethoscope to confirm bilateral air entry
Tube fixation device (Plaster tape)
Oral Airway
Suction Catheter
ETTUBE SIZE
Endotrachealtubes come in a number of different sizes ranging from 2.0 millimeters
(mm) to 10.5 mm in diameter.
7.5 to 9.0 mm is often used for men
6.0 - 7.5 mm is often used for women
3.0 - 3.5 mm is often used for newborns
2.5 to 3.0 mm used for premature infants.
10.
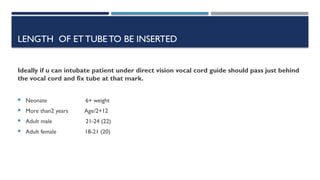
LENGTH OF ETTUBETO BE INSERTED
Ideally if u can intubate patient under direct vision vocal cord guide should pass just behind
the vocal cord and fix tube at that mark.
Neonate 6+ weight
More than2 years Age/2+12
Adult male 21-24 (22)
Adult female 18-21 (20)
11.
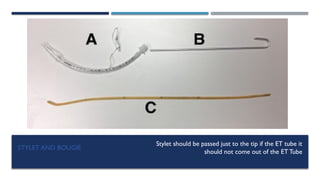
STYLET AND BOUGIE
Styletshould be passed just to the tip if the ET tube it
should not come out of the ET Tube
12.
PREPARATION
Before anendotracheal tube is placed, jewelry should be removed, especially tongue
piercings.
People should not eat or drink before surgery for at least six hours to reduce the risk
of aspiration during intubation for planned intubation such as for general anesthesia.
In case of emergency suction catheter should be available.
All the equipment that may be needed for intubation should be placed on a trolly.
Laryngoscope preferable 2 handles should be available along with different size et
tubes and stylet and bougie.
DURINGTHE PROCEDURE
Onceproper position given 100% oxygenation given for 3 minutes or in case of
conscious patient 8 vitals breaths for preoxygenation.
Laryngoscope inserted from right side of the mouth displacing tongue towards the
left.
Once epiglottis is visualized it is lifted up with laryngoscope directed upwords. As
downwards movement can break teeth.
Once vocal cords are visualized desired size ET tube is passed and laryngoscope is
removed.
Proper placement of ET tube shoed bilateral chest rise or condensation in ET tube
of can be confirmed with stethoscope.
ET tube is fixed with the plaster.
15.
COMPLICATIONS
Short term complication
Bleeding or Injury to the mouth, teeth or dental structures, tongue, thyroid gland, voice
box (larynx), vocal cords, windpipe (trachea), or esophagus.
Improper placement of the endotracheal tube into the esophagus. If this goes unnoticed,
the lack of oxygen to the body could result in brain damage, cardiac arrest, or death.
Temporary hoarseness when the tube is removed
Infection.
Pneumothorax (collapse of a lung).
Aspiration of contents of the mouth or stomach during placement which can, in turn,
16.
COMPLICATIONS
Long term complications
Tracheal stenosis, or narrowing of the trachea.
Tracheomalacia.
Spinal cord injuries.
Tracheoesophageal fistula (an abnormal passageway between the trachea and
esophagus(
Vocal cord paralysis: rare complication that can cause permanent hoarseness.