Downloaded 260 times
![DIAGNOSIS
Chief Complaint
History
[Medical/Dental]
Objective
Examination
Subjective
Examination
Radiographs](https://image.slidesharecdn.com/endodontics-anintroduction-181125110139/75/Endodontics-An-Introduction-6-2048.jpg)
![INDICATIONS
Carious teeth [caries involving
pulp]
Teeth with irreversible pulpitis
Necrotic pulps
Treatable periodontal conditions
[endo-perio lesions]
Salvageable resorptive defects
Supra-erupted teeth with good
bone support
Fractured teeth involving pulp
Intentional endodontics for FPD's
or over-dentures](https://image.slidesharecdn.com/endodontics-anintroduction-181125110139/75/Endodontics-An-Introduction-15-2048.jpg)


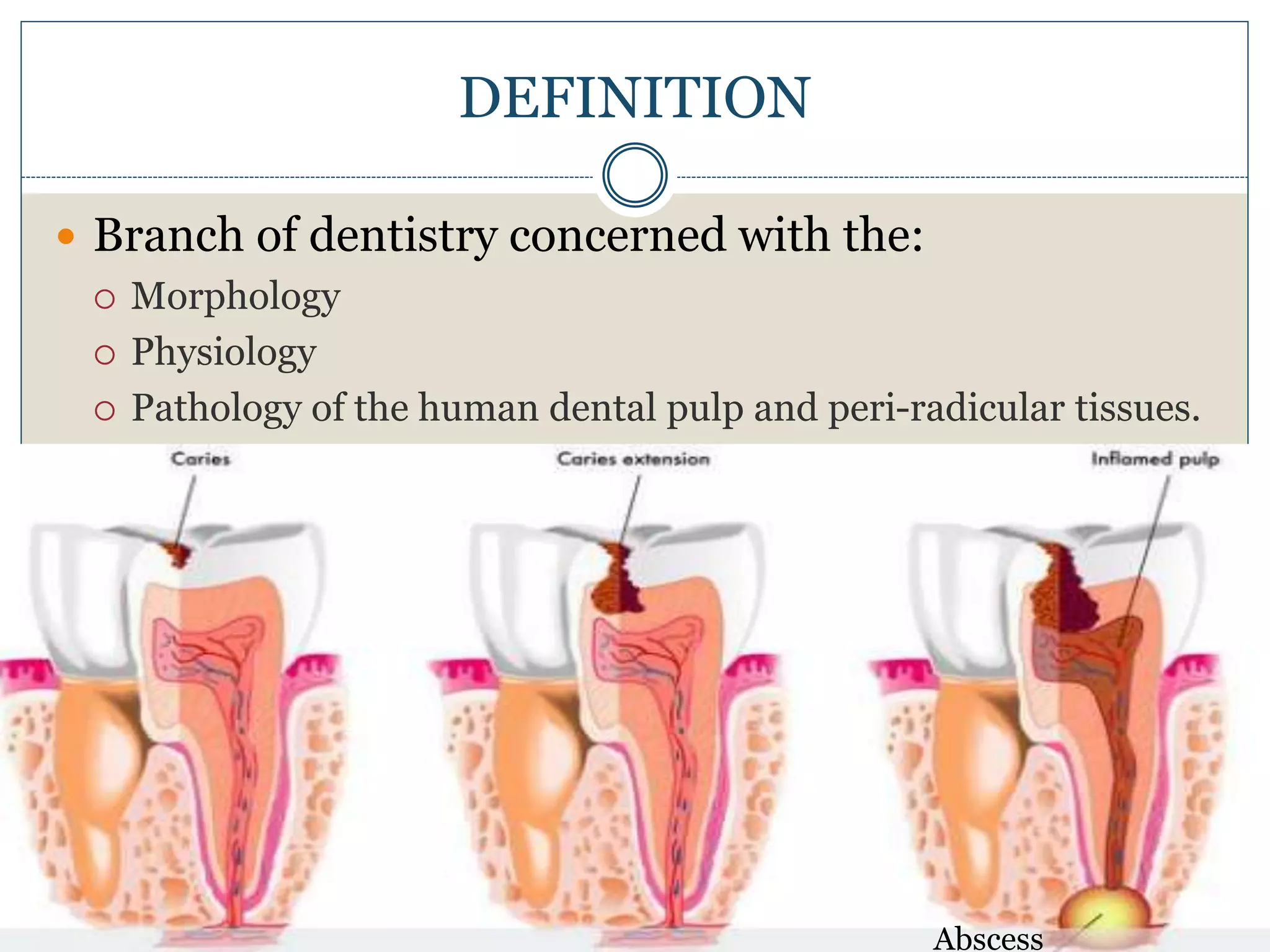
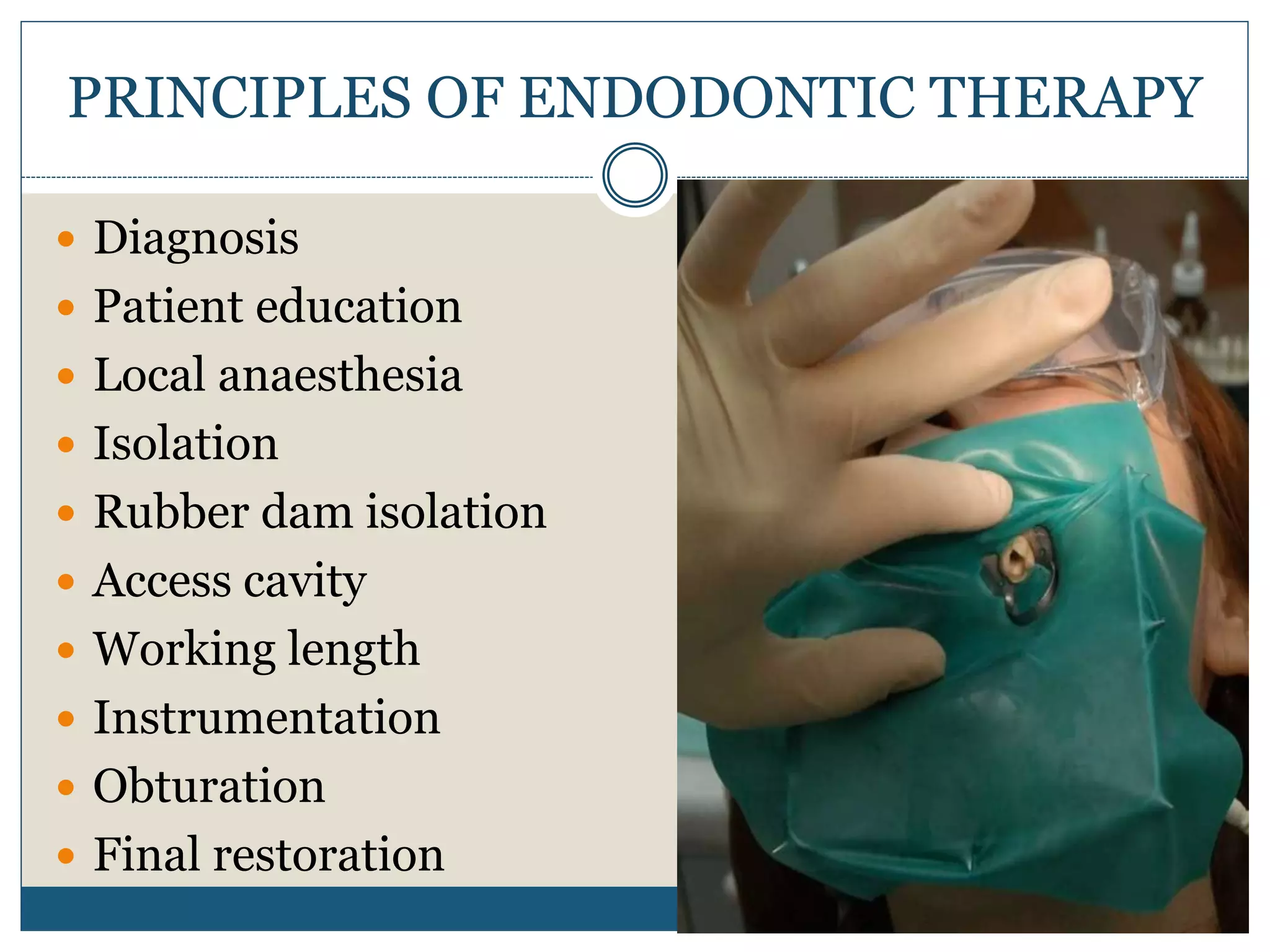
Endodontics is a branch of dentistry focused on the human dental pulp and surrounding tissues, addressing issues such as diagnosis, treatment, and prevention of pulp-related diseases. Key aspects include patient education, local anesthesia, isolation during procedures, and various techniques for canal preparation and filling. Advancements in technology and materials are expected to enhance the effectiveness of endodontic treatments in the future.




















































































