













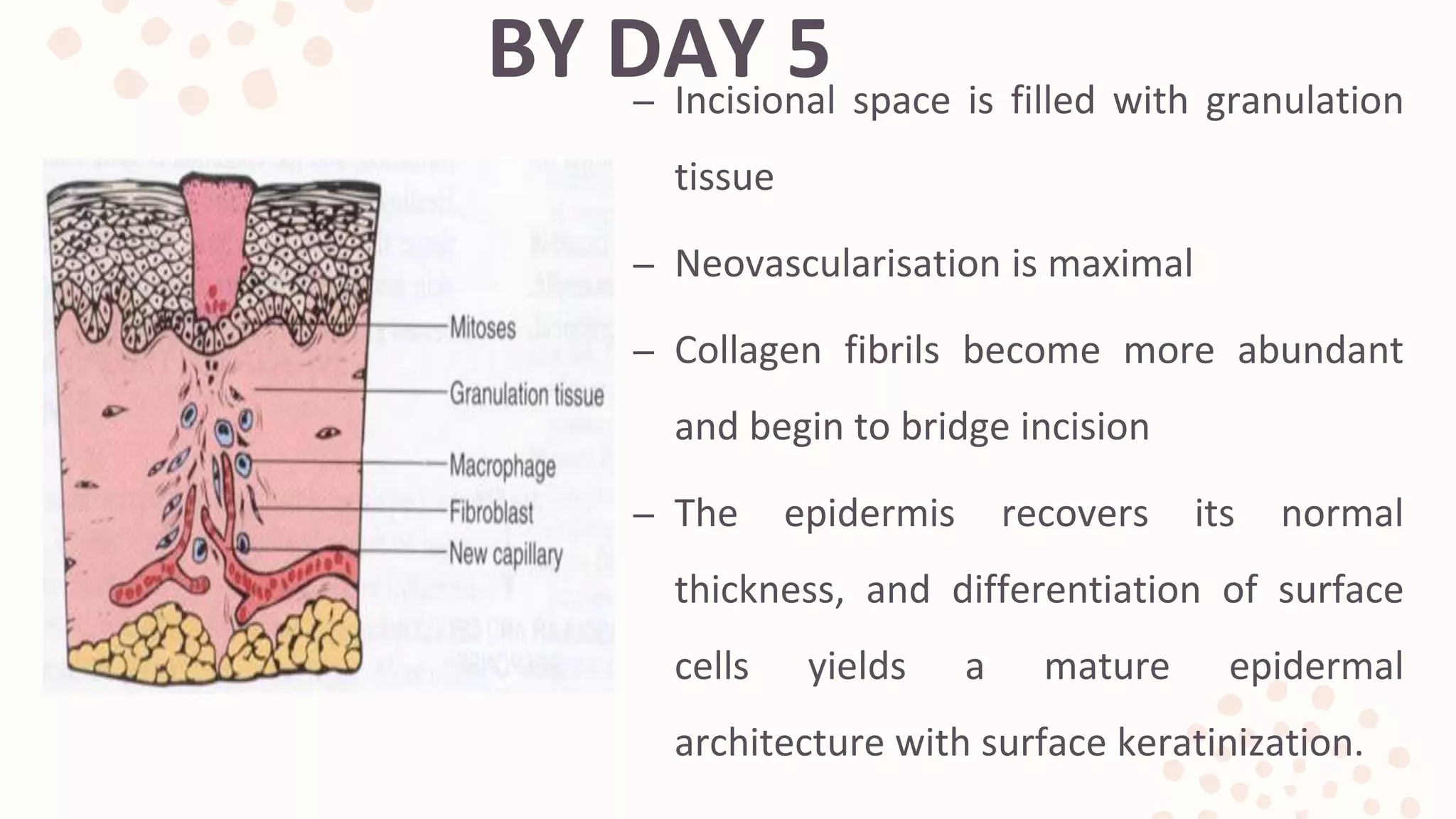















































The document discusses the phases of wound healing: 1) Hemostasis and inflammation occurs within the first few days as the wound clots and immune cells clear debris. 2) Proliferation spans days 4-12 as new tissue is formed through fibroblast and endothelial cell proliferation and migration. Collagen and new blood vessels are deposited. 3) Maturation and remodeling can take months as the wound contracts and collagen is reorganized and remodeled, increasing strength of the healed tissue.




















































































