Downloaded 458 times
![PROCEDURE
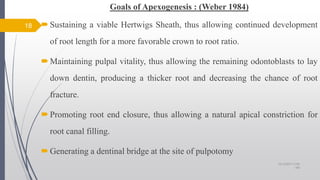
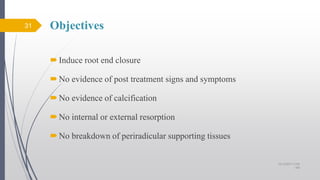
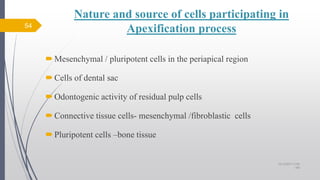
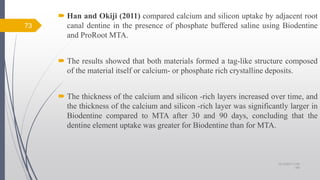
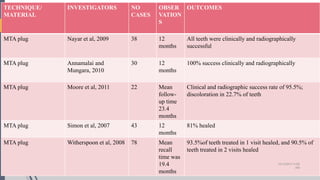
Bleeding of the pulp stump was controlled with saline on a cotton pellet
applied with gentle pressure.
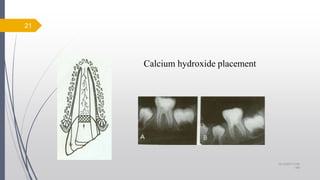
[Ca(OH)2]: Calcium hydroxide powder was mixed with saline to a thick
consistency. The paste was carefully placed on the pulp stump surface 1 to 2
mm thick.
20
Removal of coronal pulp Haemostasis
10/12/2017 4:59
AM](https://image.slidesharecdn.com/apexificationandapexogenesis-171012045915/85/Apexification-and-apexogenesis-20-320.jpg)
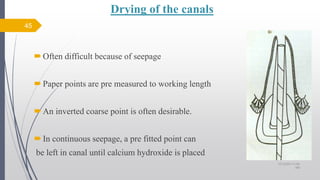

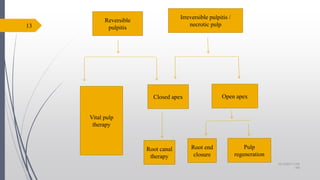
This document discusses apexification and apexogenesis procedures for immature teeth with open apices. It defines open apices as teeth with arrested root development resulting in a large apical opening. For teeth with vital pulp but pulp exposure, the goal is apexogenesis to allow continued root development through calcium hydroxide pulpotomy. For teeth with non-vital pulp, apexification is used to induce apical closure with materials like calcium hydroxide or MTA to create an apical plug for filling. Successful outcomes depend on follow up over 1-2 years to monitor continued root development or closure of the apex.











































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


