
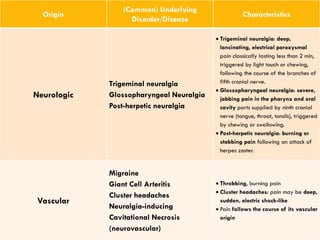
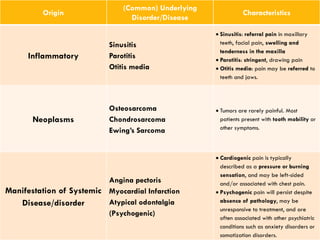

The document discusses the diagnostic processes in endodontics, highlighting the importance of accurate diagnosis for effective treatment. It covers various types of pulpal and periapical diagnoses, pain characteristics, referral patterns, and the necessity of thorough patient history and clinical examinations. Additionally, it outlines diagnostic aids and the significance of systematic data analysis to arrive at a reliable diagnosis, which guides subsequent treatment planning.










































![endo diagnosis ppt friday.pptx [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/endodiagnosispptfriday-240220084902-bcb16ad0-thumbnail.jpg?width=640&height=640&fit=bounds)

































