Download to read offline
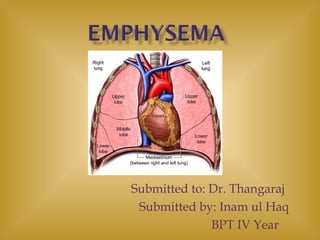
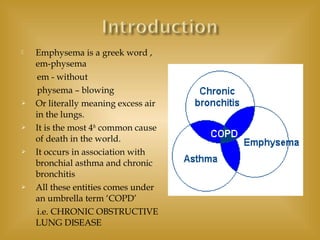
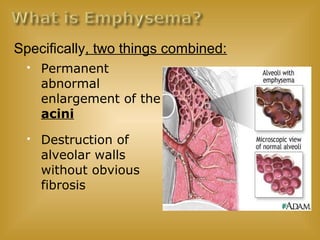




















Emphysema is a chronic lung disease characterized by destruction of the alveoli, or air sacs, in the lungs. It causes shortness of breath and occurs most often due to long-term smoking. The document discusses the definition, causes, risk factors, symptoms, diagnosis, and treatment of emphysema. Treatment options include quitting smoking, oxygen therapy, medications like bronchodilators and corticosteroids, and potentially lung surgery for severe cases.