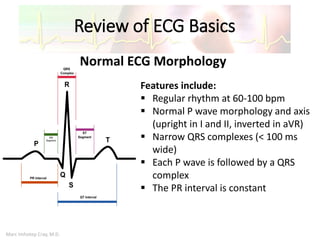
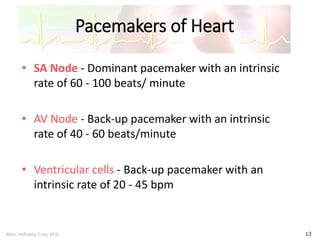
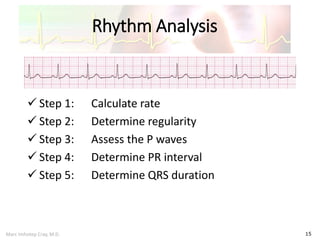
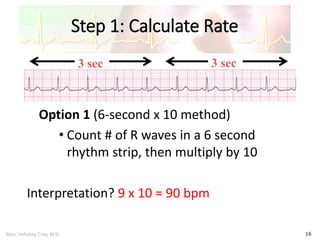
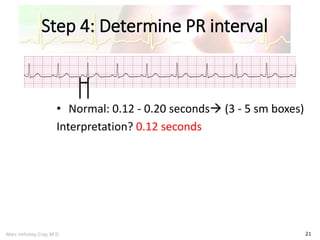
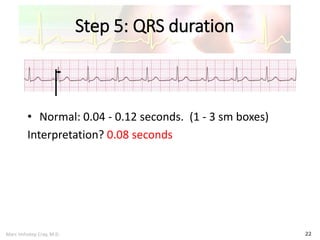
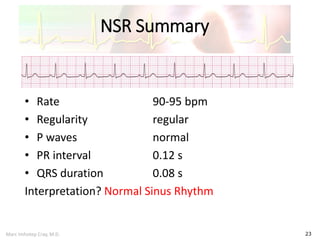
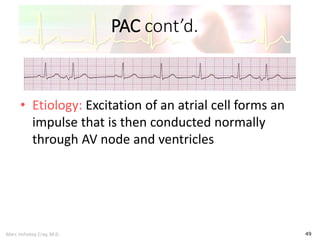
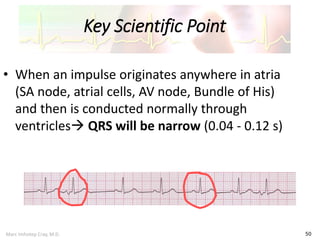
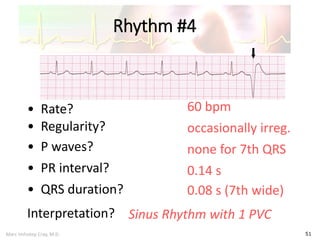
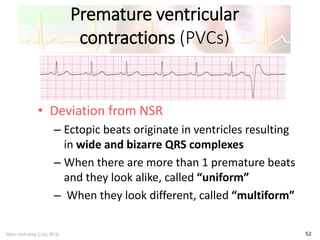
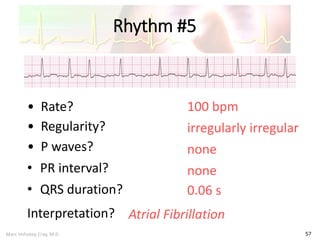
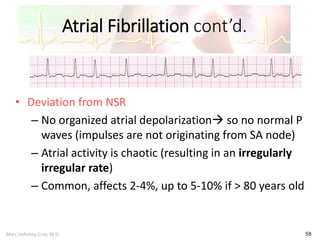
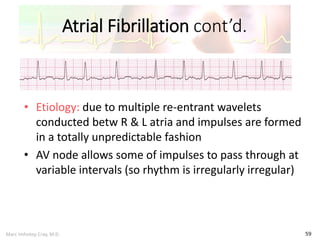
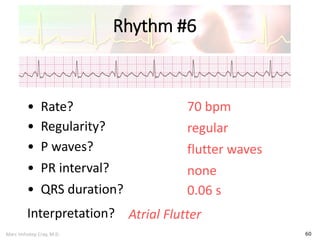
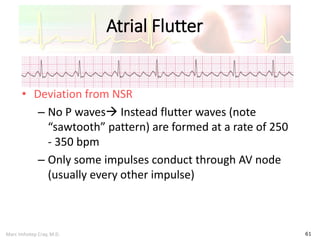
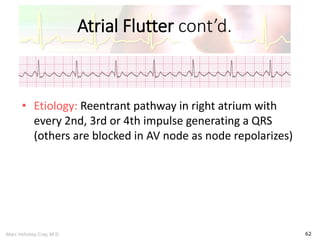
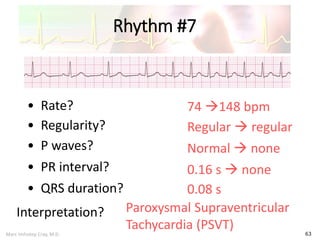
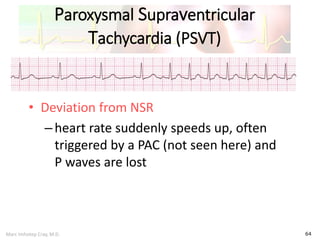
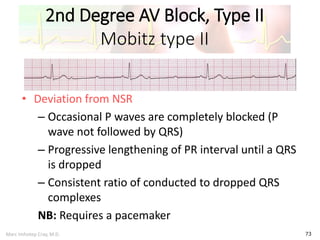
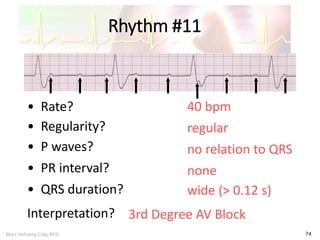
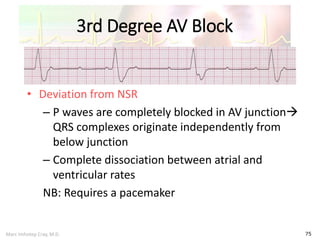
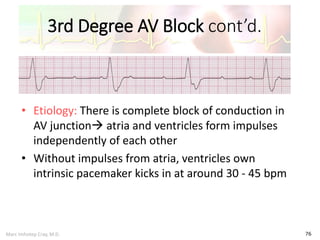
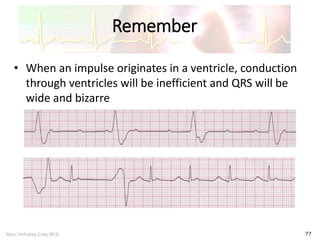
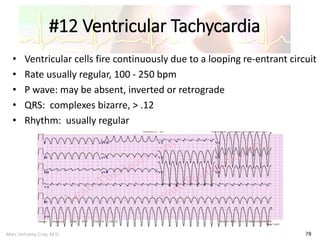
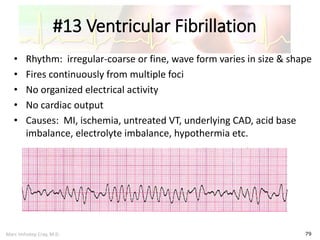
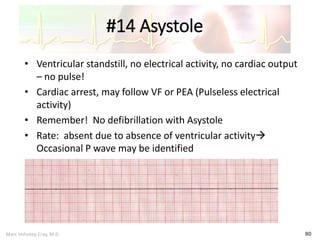



This document provides an overview of electrocardiogram (ECG) interpretation. It begins by outlining the learning objectives, which are to recognize normal sinus rhythm, common rhythm disturbances on a 3-lead ECG, and how to interpret a myocardial infarction on a 12-lead ECG. The document then reviews ECG basics, how to analyze rhythms, defines normal sinus rhythm, and discusses common cardiac dysrhythmias and how to diagnose a myocardial infarction. It provides examples of various normal and abnormal rhythms.