Downloaded 536 times












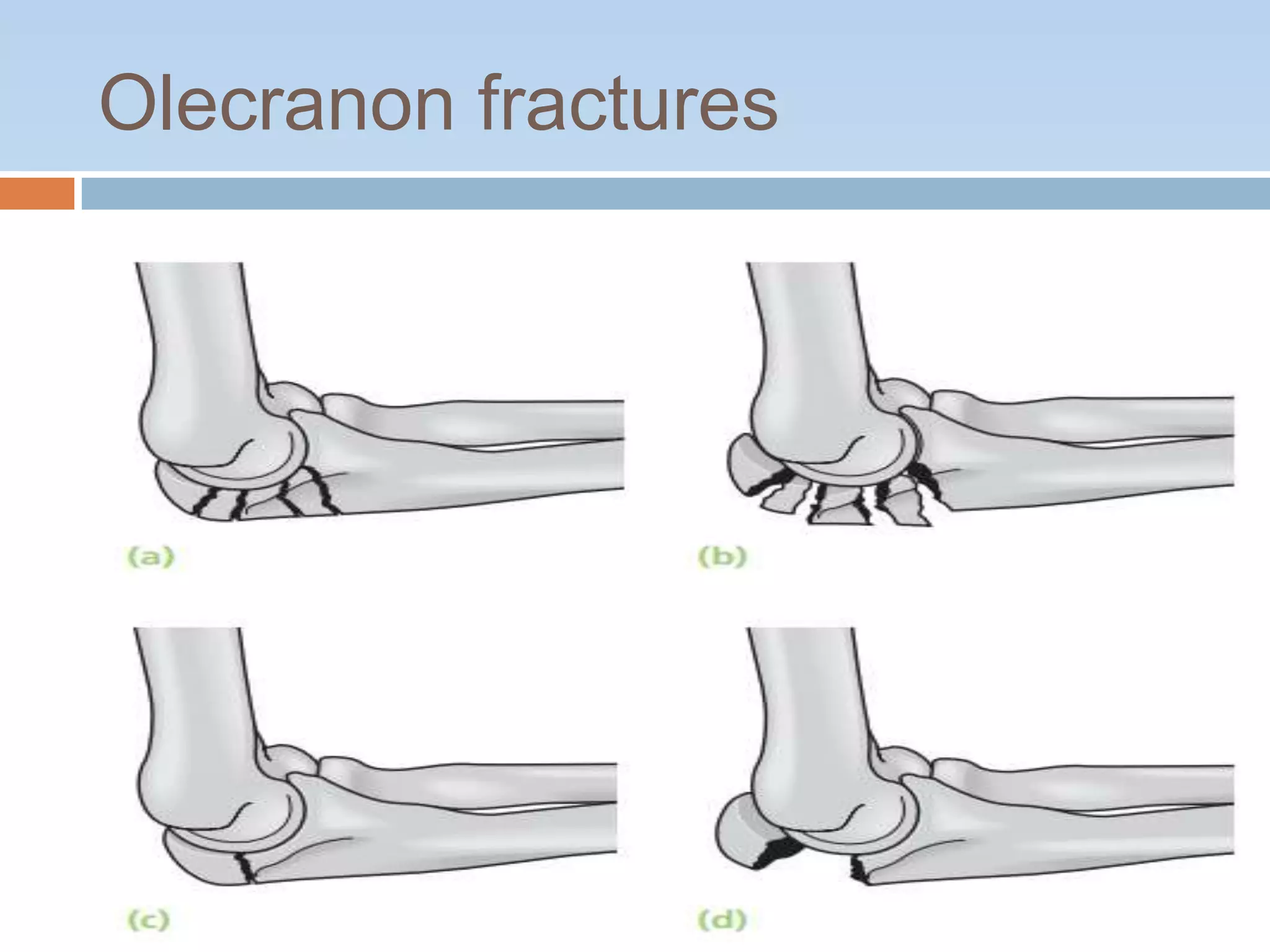











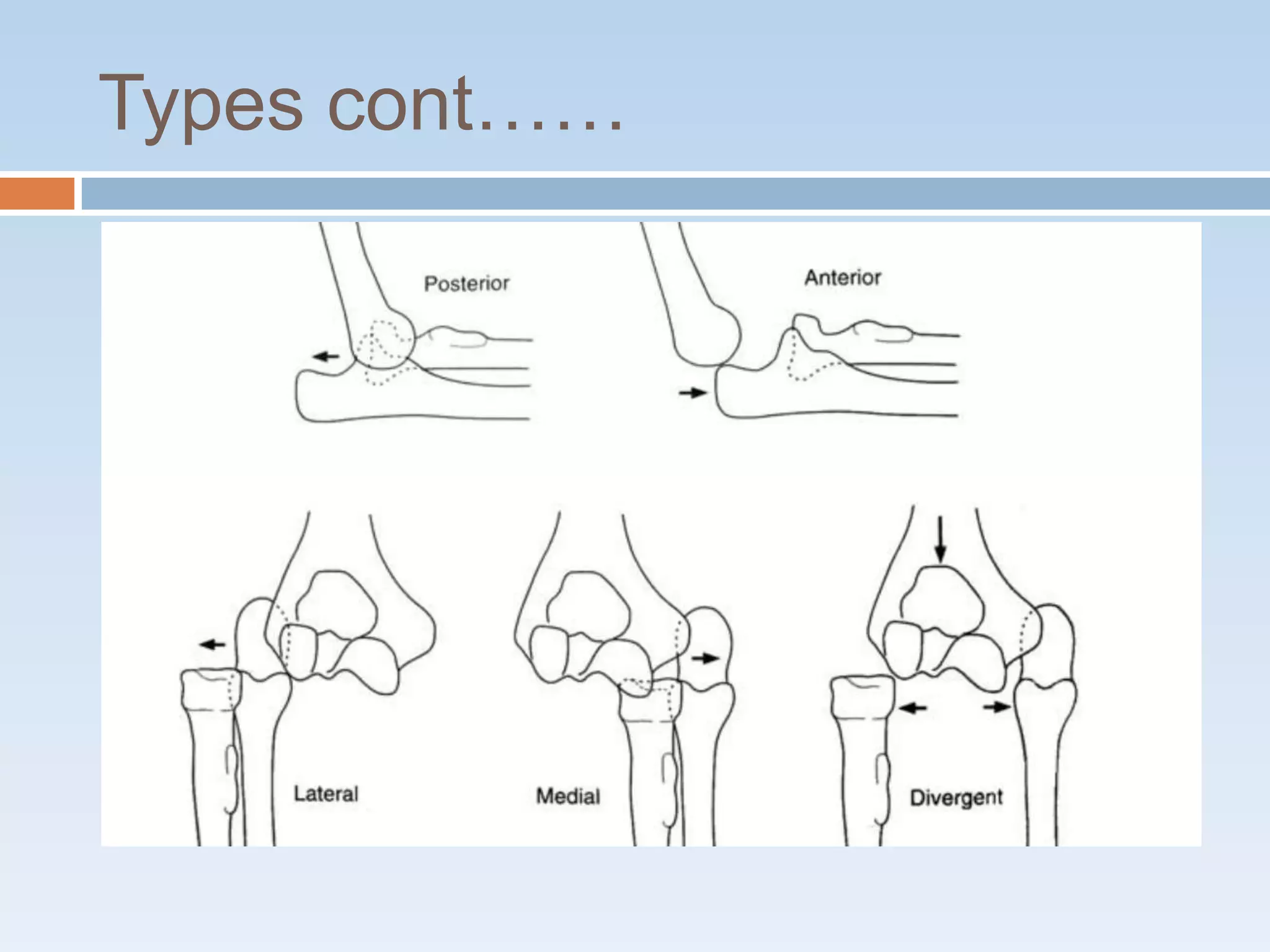







This document discusses elbow fractures and dislocations. It begins by classifying various types of elbow fractures including intercondyler fractures, condylar fractures, capitulum fractures, radial neck fractures, and fractures of the olecranon and coronoid processes. It then discusses classifications for many of these fractures. The document also covers elbow dislocations, describing the most common types, associated injuries, symptoms, imaging, treatment, and potential complications.























































































