Downloaded 281 times
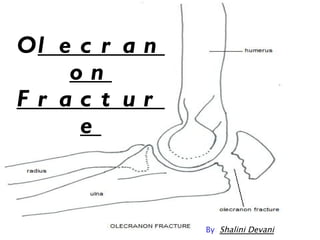


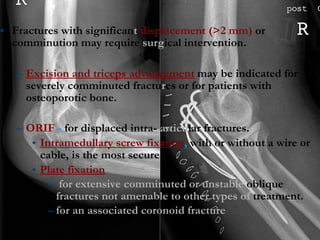
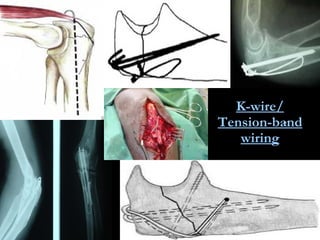
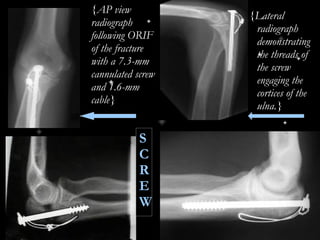
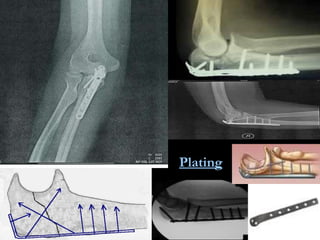

An olecranon fracture is a break of the proximal end of the ulna bone where it forms part of the elbow joint. It most often occurs from a fall on an outstretched arm. Diagnosis is made through physical exam finding tenderness and a gap at the fracture site as well as x-rays. Treatment depends on the severity of the break, with minor fractures treated by casting and more severe displaced fractures requiring surgical fixation such as screws, plates or wires to stabilize the bone fragments. Complications can include stiffness, non-healing of the fracture and arthritis if not properly treated.























































































