Downloaded 295 times
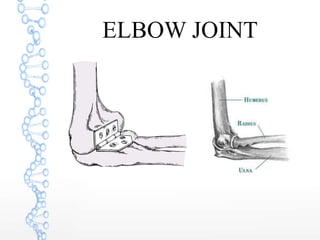
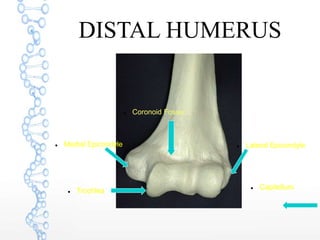
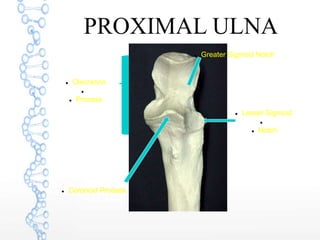
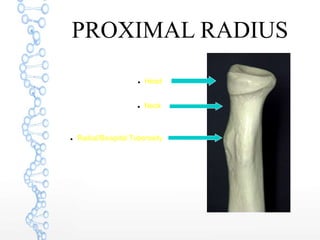
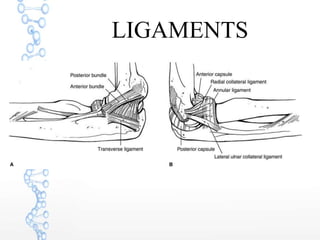
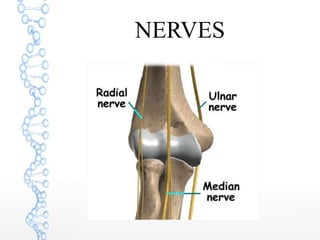






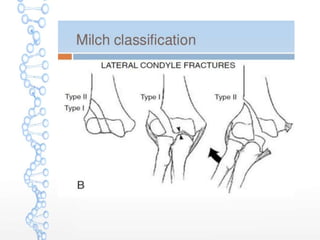
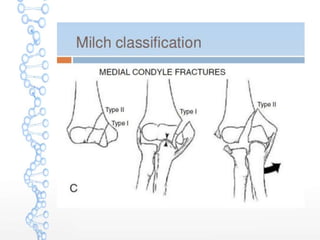






This document discusses distal humerus fractures and elbow dislocations. It begins with anatomy of the elbow joint and then describes the classification, clinical features, imaging, treatment and complications of distal humerus fractures. These fractures have two peak incidence ages and most common types involve one or two columns of the elbow. Treatment depends on factors like displacement and patient age. Elbow dislocations also have associated injuries and mechanisms described. Closed reduction is usually attempted initially but surgery may be needed for unstable or complex cases. Complications of both include stiffness, neurological issues and post-traumatic arthritis.



































































