Downloaded 759 times
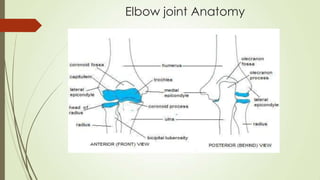
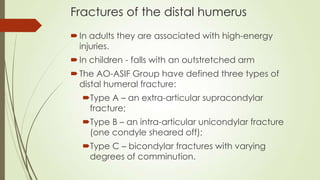
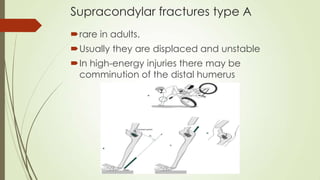
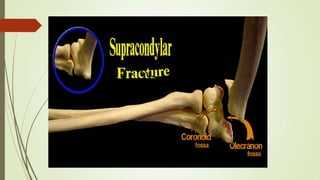



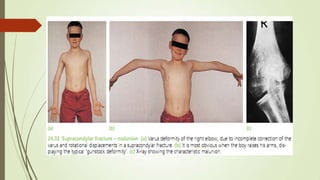
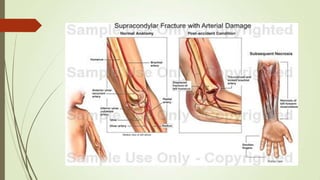
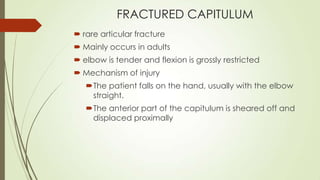
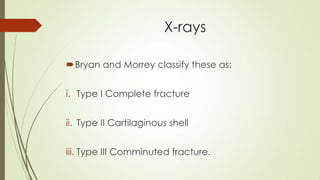
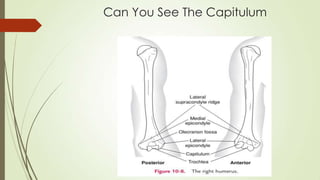
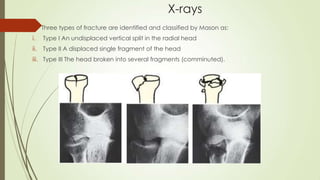
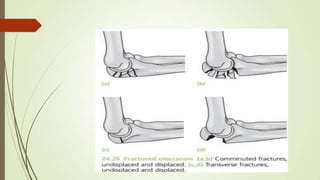











This document discusses fractures of the elbow and forearm. It describes the anatomy of the elbow joint and various types of fractures that can occur in the distal humerus, radial head, coronoid process, and olecranon. Treatment options for different fracture patterns include closed reduction, open reduction and internal fixation using plates, screws and tension band wiring. Complications like stiffness, non-union and nerve injuries are also discussed. Physiotherapy management aims to regain range of motion, muscle strength, and function.









































































