Downloaded 339 times

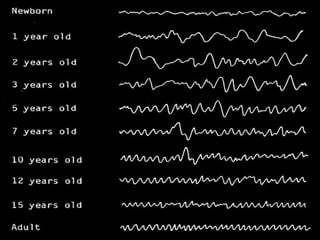


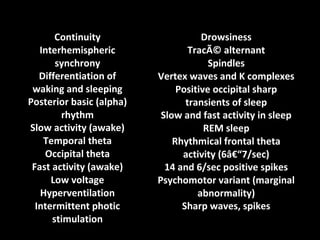
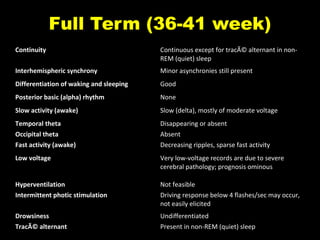


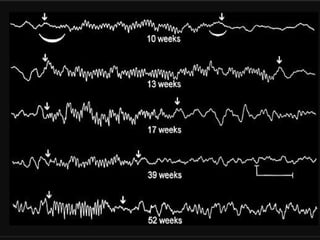
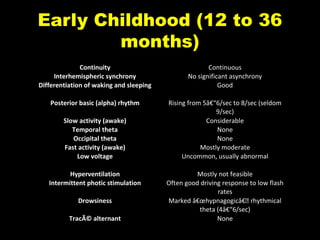
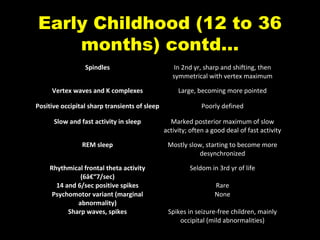
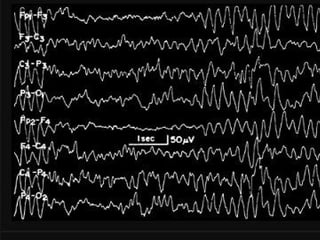
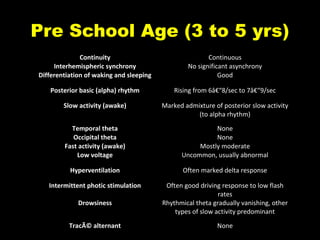
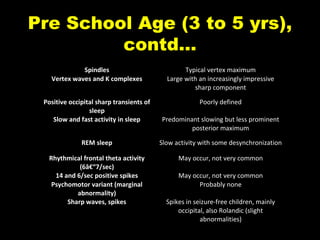

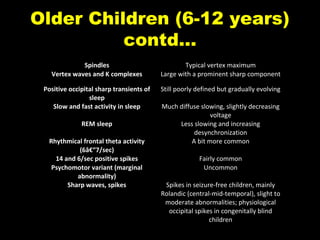
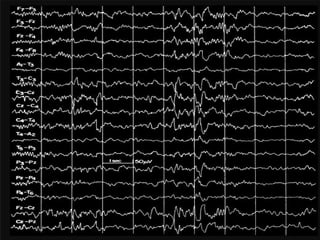

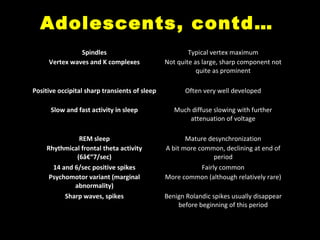
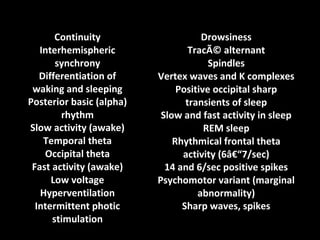

The document discusses the maturation of EEG patterns from infancy to adolescence, detailing changes in interhemispheric synchrony, differentiation between waking and sleeping states, and various brainwave activities at different developmental stages. It describes the development of alpha rhythms, theta activity, and spikes, as well as their significance in terms of normalcy and pathology. The document highlights specific EEG characteristics during infancy, early childhood, preschool age, older children, and adolescents, emphasizing the evolution of brain activity patterns over time.








































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









