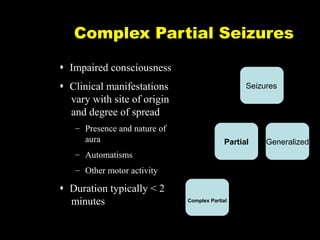
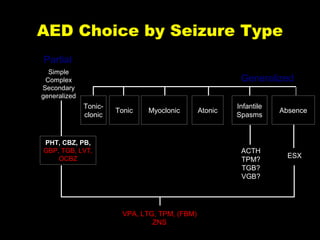
Complex Partial Seizures
Impaired consciousness
Clinical manifestations
vary with site of origin
and degree of spread
– Presence and nature of
aura
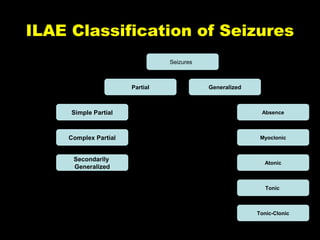
Seizures
Partial
Generalized
– Automatisms
– Other motor activity
Duration typically < 2
minutes
Complex Partial
C-Slide 3
Influence on Hepatic
Metabolism
•1st Generation antiepileptic drugs
– Inducers
• Phenobarbital
• Phenytoin
• Carbamazepine
– Inhibitor
• Valproate
• Therefore, affect the kinetics and dynamics of nonCNS drugs as well…
14.
DO WE NEEDMORE NEW
ANTIEPILEPTIC DRUGS?
• Problem with conventional AEDs:
– Seizure control
• Newly diagnosed well treated
• Still 40% with therapy resistance
• New AEDs over last 20 years are slowly
changing this equation!
15.
The Ideal AEDTherapy:
• Improved efficacy → no seizures
• Few side effects → no new problems in
patient’s daily life
• Easy dosing scheduling → no chance for
dosing mistakes
• Minimal drug interactions → no need to
adjust other medicines
• Expense not prohibitive → cost will not
prevent taking the AED
• Maximizing quality of life
16.
New Versus StandardAEDs
• Equal efficacy
• Differentiated by
– Adverse events
– Drug interactions
– Pharmacokinetics profiles
17.
How do wemake progress?
• Revolutionary Drugs
– Drugs that work with new mechanisms never tried
before
– Expectation: They will control seizures that
existing drugs can’t control
• Evolutionary Drugs
– Improve on existing drugs
– Expectation: We can eliminate some of the
problems/side effects of good drugs, without
reducing their effect on seizures
18.
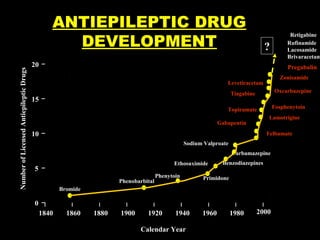
Number of LicensedAntiepileptic Drugs
ANTIEPILEPTIC DRUG
DEVELOPMENT
?
20
Pregabalin
Zonisamide
Levetiracetam
Oxcarbazepine
Tiagabine
15
Fosphenytoin
Topiramate
Lamotrigine
Gabapentin
10
Felbamate
Sodium Valproate
Carbamazepine
Ethosuximide
5
Phenobarbital
Phenytoin
Benzodiazepines
Primidone
Bromide
0
1840
Retigabine
Rufinamide
Lacosamide
Brivaracetam
1860
1880
1900
1920
1940
Calendar Year
1960
1980
2000
19.
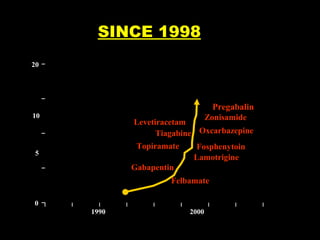
Number of LicensedAntiepileptic Drugs
SINCE 1998
20
Pregabalin
10
Zonisamide
Levetiracetam
Tiagabine Oxcarbazepine
Topiramate
5
Fosphenytoin
Lamotrigine
Gabapentin
Felbamate
0
1990
2000
Calendar Year
Gabapentin
• Mechanism
– designed,yet unknown
• Dose (900 to 4800 mg/day [TID to QID])
• Side Effects
– fatigue, dizziness, ataxia
• Drug Interactions
– None with AEDs [only Antacids]
• Renal Elimination - CrCl
• Clinical Pearl
– non-Epilepsy uses
22.
Lamotrigine
• Mechanism
– Na+Channels, Glutamate
• Dose (100 to 500 mg/day [QD or BID])
• Side Effects
– Sedation, Diplopia, Ataxia, Nausea - Rash
• Drug Interactions
• “one way street”
• Contraceptives
• Clinical Pearl
• Slow taper - (esp. VPA)
• Incidence of severe rash may by overestimated
• Pediatric approval
23.
Topiramate
• Mechanisms -many
– Na+ Channels, Glutamate, GABA, CAI
• Dose (200 to 400 mg/day [BID - QDrenal])
• Side Effects
• Sedation, Difficulty Concentrating, Kidney Stones, Glaucoma
• Drug Interactions
– “one way street”
• Clinical Pearl
– ceiling dose, fluids, visual changes, use outside of
epilepsy
24.
Tiagabine
• Mechanism
– Blocksre-uptake of pre-synaptic GABA
• Dose (32 to 56 mg/day [BID to QID])
• Side Effects
– Fatigue, Dizziness, Weakness
• Drug Interactions
– “one-way street”
• Clinical Pearl
• different mechanism of action
• take with food to decrease side effects (same AUC)
25.
Oxcarbazepine
• Mechanism -Na+ Channels
• Dose
• Adjunctive (600 to 1,200 mg/day [BID])
• Mono (up to 2,400 mg/day)
• Side Effects
• Dizziness, Somnolence, Diplopia, N/V, Ataxia
• Drug Interactions
• Inhibit/Induce - OCs, PHT
• Clinical Pearl
• Prodrug (OCBZ to MHD)
26.
Levetiracetam
• Mechanism
– SV2 inhibitor
• Dose: (1,000 to 3,000 mg/day [BID])
• Side Effects
– Somnolence, Asthenia, Infection, Dizziness
• Drug Interactions
– PK
• None with AEDs, probenecid - metabolite
– PD ?
• Clinical Pearl
– Adjust dose for renal function
27.
Zonisamide
• Mechanism
– Na+and T-calcium channels, CAI
• Dose: 100 to 600 mg/day (BID or QD)
• Side Effects:
– somnolence, dizziness, nausea, headache,
agitation/irritation, kidney stones, weight loss
• Drug Interactions
• No effect on others
• Clinical Pearl
• Appr. Japan & Korea ‘89, Sulfonamide
• Use outside of epilepsy
28.
What’s really new
•Two new drugs
– Revolutionary
• lacosamide
• rufinamide
• Four drugs in late trials
– Evolutionary
• brivaracetam
• Eslicarbazepine
– Revolutionary:
• Carisbamate
• Retigabine
29.
Lacosamide
• Works onsodium channels, like
Carbamazepine and Phenytoin
• However, It selectively enhances slow
inactivation of sodium channels, whereas the
older drugs work on fast inactivation
• Approved in Europe and USA
30.
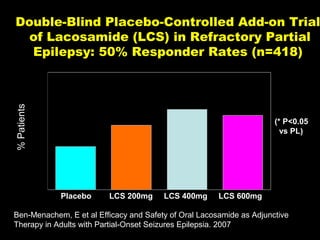
Double-Blind Placebo-Controlled Add-onTrial
of Lacosamide (LCS) in Refractory Partial
Epilepsy: 50% Responder Rates (n=418)
% Patients
41%*
38%*
33%
(* P<0.05
vs PL)
22%
Placebo
LCS 200mg
LCS 400mg
LCS 600mg
Ben-Menachem, E et al Efficacy and Safety of Oral Lacosamide as Adjunctive
Therapy in Adults with Partial-Onset Seizures Epilepsia. 2007
31.
RUFINAMIDE
• Also workson sodium channels with new
mechanism
• Approved in Europe for treatment of a severe
form of epilepsy (Lennox-Gastaut syndrome)
– “Orphan drug”
• In Front of FDA for Lennox-Gastaut and
Partial seizures
32.
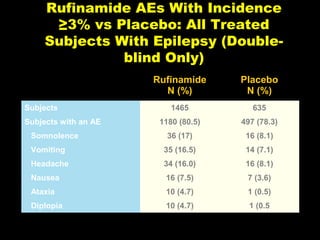
Rufinamide AEs WithIncidence
≥3% vs Placebo: All Treated
Subjects With Epilepsy (Doubleblind Only)
Rufinamide
N (%)
Placebo
N (%)
1465
635
1180 (80.5)
497 (78.3)
36 (17)
16 (8.1)
Vomiting
35 (16.5)
14 (7.1)
Headache
34 (16.0)
16 (8.1)
Nausea
16 (7.5)
7 (3.6)
Ataxia
10 (4.7)
1 (0.5)
Diplopia
10 (4.7)
1 (0.5
Subjects
Subjects with an AE
Somnolence
33.
BRIVARACETAM
• Similar mechanismto Levetiracetam but much
stronger in animal models
• Also has sodium channel blocking activity
• FDA trials underway
34.
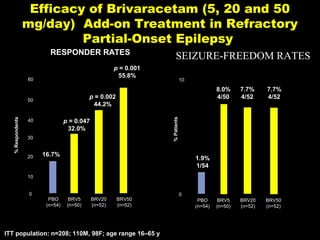
Efficacy of Brivaracetam(5, 20 and 50
mg/day) Add-on Treatment in Refractory
Partial-Onset Epilepsy
RESPONDER RATES
p = 0.001
55.8%
60
8.0%
4/50
p = 0.047
32.0%
40
7.7%
4/52
7.7%
4/52
BRV5
(n=50)
BRV20
(n=52)
BRV50
(n=52)
% Patients
% Respondents
10
p = 0.002
44.2%
50
30
20
SEIZURE-FREEDOM RATES
16.7%
1.9%
1/54
10
0
PBO
(n=54)
BRV5
(n=50)
BRV20
(n=52)
BRV50
(n=52)
ITT population: n=208; 110M, 98F; age range 16–65 y
0
PBO
(n=54)
35.
Eslicarbazepine
• A “thirdgeneration” Carbamazepine
• Improves on second generation
– Less effect on sodium
– Smoother release may produce less side effects
• Hopefully will work equally as well
• Ready to submit to FDA
36.
•
•
•
•
Summary of 2ndGeneration
AEDs
Safer
More expensive
May help with intractable partial seizures
Less drug interactions
• Not profoundly more potent
37.
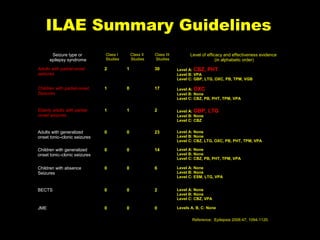
ILAE Summary Guidelines
Seizuretype or
epilepsy syndrome
Class I
Studies
Class II
Studies
Class III
Studies
Level of efficacy and effectiveness evidence
(in alphabetic order)
Adults with partial-onset
seizures
2
1
30
Level A: CBZ, PHT
Level B: VPA
Level C: GBP, LTG, OXC, PB, TPM, VGB
Children with partial-onset
Seizures
1
0
17
Level A: OXC
Level B: None
Level C: CBZ, PB, PHT, TPM, VPA
Elderly adults with partialonset seizures
1
1
2
Level A: GBP,
Level B: None
Level C: CBZ
Adults with generalized
onset tonic–clonic seizures
0
0
23
Level A: None
Level B: None
Level C: CBZ, LTG, OXC, PB, PHT, TPM, VPA
Children with generalized
onset tonic–clonic seizures
0
0
14
Level A: None
Level B: None
Level C: CBZ, PB, PHT, TPM, VPA
Children with absence
Seizures
0
0
6
Level A: None
Level B: None
Level C: ESM, LTG, VPA
BECTS
0
0
2
Level A: None
Level B: None
Level C: CBZ, VPA
JME
0
0
0
Levels A, B, C: None
LTG
Reference: Epilepsia 2006:47; 1094-1120.
38.
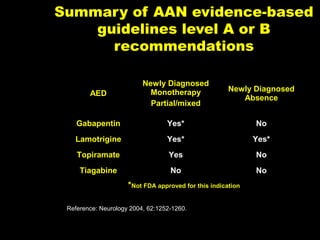
Summary of AANevidence-based
guidelines level A or B
recommendations
AED
Newly Diagnosed
Monotherapy
Partial/mixed
Newly Diagnosed
Absence
Gabapentin
Yes*
No
Lamotrigine
Yes*
Yes*
Topiramate
Yes
No
Tiagabine
No
No
*Not FDA approved for this indication
Reference: Neurology 2004, 62:1252-1260.
C-Slide 38
39.
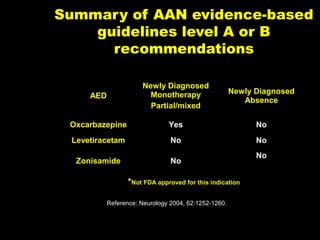
Summary of AANevidence-based
guidelines level A or B
recommendations
AED
Newly Diagnosed
Monotherapy
Partial/mixed
Newly Diagnosed
Absence
Oxcarbazepine
Yes
No
Levetiracetam
No
No
Zonisamide
No
No
*Not FDA approved for this indication
Reference: Neurology 2004, 62:1252-1260.
C-Slide 39
40.
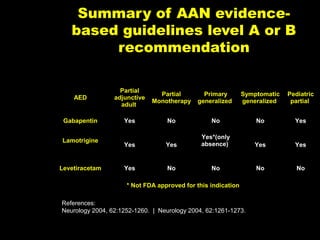
Summary of AANevidencebased guidelines level A or B
recommendation
AED
Partial
adjunctive
adult
Partial
Monotherapy
Primary
generalized
Symptomatic
generalized
Pediatric
partial
Gabapentin
Yes
No
No
No
Yes
Yes
Yes
Yes*(only
absence)
Yes
Yes
Yes
No
No
No
No
Lamotrigine
Levetiracetam
* Not FDA approved for this indication
References:
Neurology 2004, 62:1252-1260. | Neurology 2004, 62:1261-1273.
C-Slide 40
41.
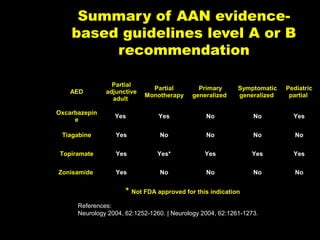
Summary of AANevidencebased guidelines level A or B
recommendation
AED
Partial
adjunctive
adult
Partial
Monotherapy
Primary
generalized
Symptomatic
generalized
Pediatric
partial
Oxcarbazepin
e
Yes
Yes
No
No
Yes
Tiagabine
Yes
No
No
No
No
Topiramate
Yes
Yes*
Yes
Yes
Yes
Zonisamide
Yes
No
No
No
No
* Not FDA approved for this indication
References:
Neurology 2004, 62:1252-1260. | Neurology 2004, 62:1261-1273.
C-Slide 41
42.
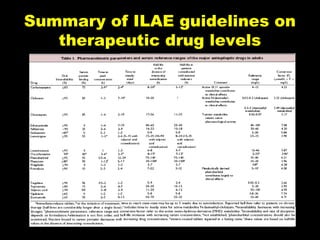
Summary of ILAEguidelines on
therapeutic drug levels
C-Slide 42
#4 Complex partial seizures impair consciousness. Typically, staring is accompanied by impaired responsiveness, cognitive function, and recall, although some degree of responsiveness may be preserved (e.g., orienting toward a stimulus). Automatic movements (automatisms) are common and involve the mouth (e.g., lip smacking, chewing, swallowing), upper extremities (e.g., fumbling, picking), vocalization/verbalization (e.g., grunts, repeating a phrase), or complex acts (e.g., shuffling cards). More dramatic automatisms occasionally occur (e.g., screaming, running, disrobing, pelvic thrusting). Complex partial seizures usually last from 15 seconds to 3 minutes. After the seizure, postictal confusion is common, usually lasting less than 15 minutes, although other symptoms, such as fatigue, may persist for hours.
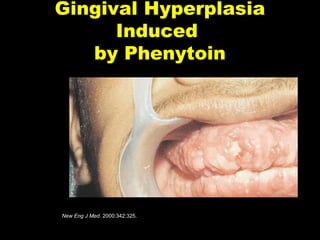
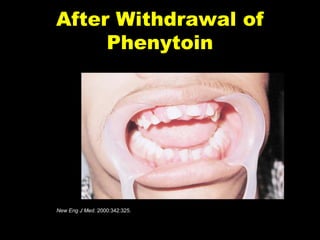
#10 17 yo boy with h/o generalized tonic clonic seizures for 4 years on phenytoin 300mg/day for 2 years WITHOUT SUPERVISION.
Found to have severe gingival hyperplasia and cerebellar ataxia.
#40 These slides really on a more complicated level than rest of talk

![Gabapentin
• Mechanism
– designed, yet unknown
• Dose (900 to 4800 mg/day [TID to QID])
• Side Effects
– fatigue, dizziness, ataxia
• Drug Interactions
– None with AEDs [only Antacids]
• Renal Elimination - CrCl
• Clinical Pearl
– non-Epilepsy uses](https://image.slidesharecdn.com/aednewvsoldfinal-140130012303-phpapp02/85/Aed-new-vs-old-final-21-320.jpg)
![Lamotrigine
• Mechanism
– Na+ Channels, Glutamate
• Dose (100 to 500 mg/day [QD or BID])
• Side Effects
– Sedation, Diplopia, Ataxia, Nausea - Rash
• Drug Interactions
• “one way street”
• Contraceptives
• Clinical Pearl
• Slow taper - (esp. VPA)
• Incidence of severe rash may by overestimated
• Pediatric approval](https://image.slidesharecdn.com/aednewvsoldfinal-140130012303-phpapp02/85/Aed-new-vs-old-final-22-320.jpg)
![Topiramate
• Mechanisms - many
– Na+ Channels, Glutamate, GABA, CAI
• Dose (200 to 400 mg/day [BID - QDrenal])
• Side Effects
• Sedation, Difficulty Concentrating, Kidney Stones, Glaucoma
• Drug Interactions
– “one way street”
• Clinical Pearl
– ceiling dose, fluids, visual changes, use outside of
epilepsy](https://image.slidesharecdn.com/aednewvsoldfinal-140130012303-phpapp02/85/Aed-new-vs-old-final-23-320.jpg)
![Tiagabine
• Mechanism
– Blocks re-uptake of pre-synaptic GABA
• Dose (32 to 56 mg/day [BID to QID])
• Side Effects
– Fatigue, Dizziness, Weakness
• Drug Interactions
– “one-way street”
• Clinical Pearl
• different mechanism of action
• take with food to decrease side effects (same AUC)](https://image.slidesharecdn.com/aednewvsoldfinal-140130012303-phpapp02/85/Aed-new-vs-old-final-24-320.jpg)
![Oxcarbazepine
• Mechanism - Na+ Channels
• Dose
• Adjunctive (600 to 1,200 mg/day [BID])
• Mono (up to 2,400 mg/day)
• Side Effects
• Dizziness, Somnolence, Diplopia, N/V, Ataxia
• Drug Interactions
• Inhibit/Induce - OCs, PHT
• Clinical Pearl
• Prodrug (OCBZ to MHD)](https://image.slidesharecdn.com/aednewvsoldfinal-140130012303-phpapp02/85/Aed-new-vs-old-final-25-320.jpg)
![Levetiracetam
• Mechanism
– SV 2 inhibitor
• Dose: (1,000 to 3,000 mg/day [BID])
• Side Effects
– Somnolence, Asthenia, Infection, Dizziness
• Drug Interactions
– PK
• None with AEDs, probenecid - metabolite
– PD ?
• Clinical Pearl
– Adjust dose for renal function](https://image.slidesharecdn.com/aednewvsoldfinal-140130012303-phpapp02/85/Aed-new-vs-old-final-26-320.jpg)


































































![new or old AEDs new [Autosaved] - Copy.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/neworoldaedsnewautosaved-copy-241218172407-66b2b33d-thumbnail.jpg?width=640&height=640&fit=bounds)