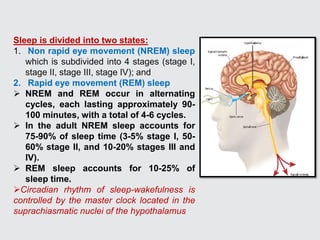
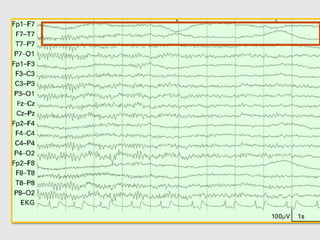
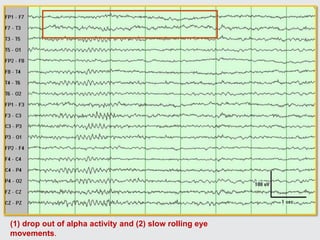
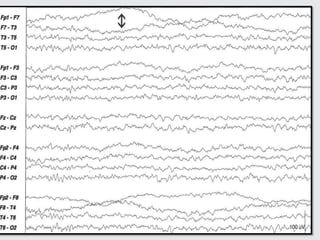
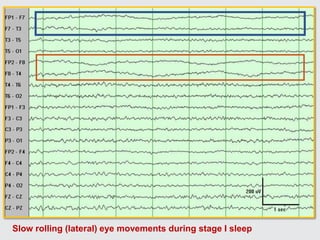
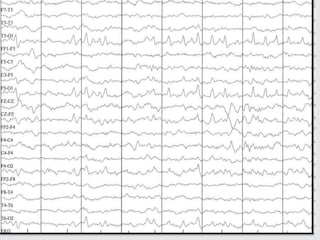
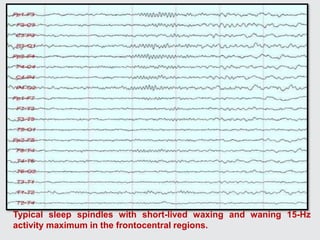
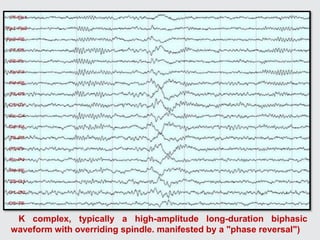
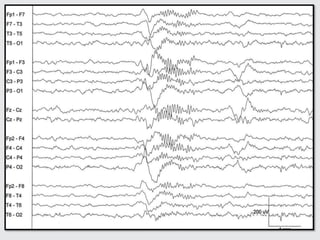
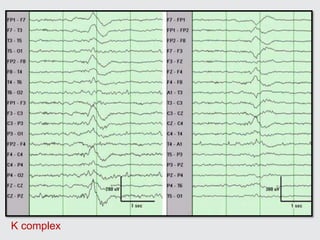
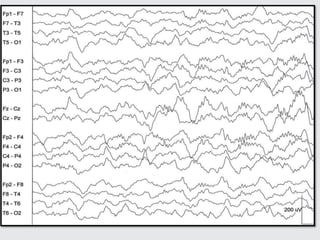
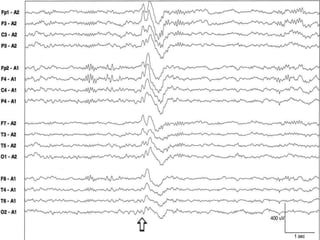
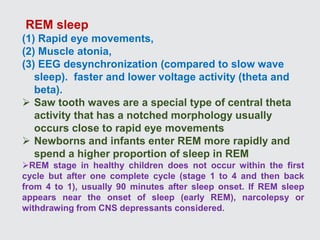
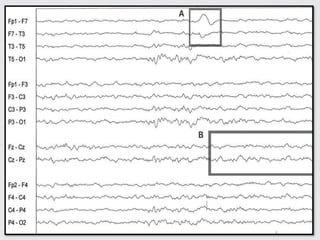
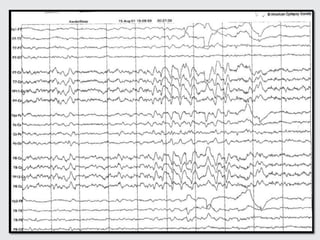
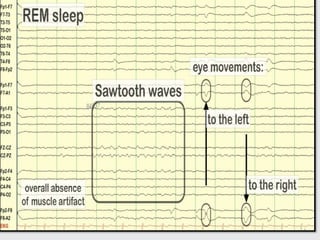
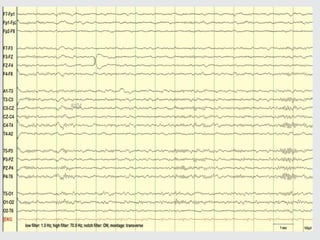
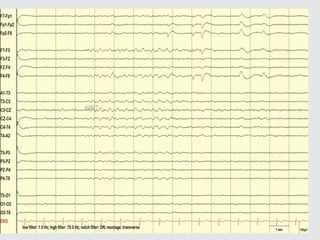
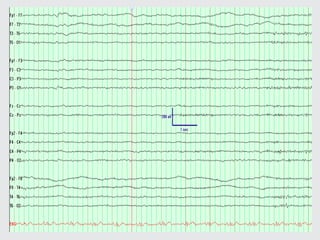
This document summarizes the effects of sleep on EEG patterns. It describes the typical EEG patterns seen in each sleep stage, including: slow rolling eye movements and alpha attenuation in stage 1; sleep spindles, K-complexes, and vertex waves in stage 2; predominant delta activity in stages 3 and 4; and EEG desynchronization along with rapid eye movements in REM sleep. Key findings are outlined for each stage to characterize normal EEG changes that occur during the sleep cycle.